

Immune Checkpoint Inhibitors for Microsatellite Instability High Unresectable Obstructive Colon Cancer: A Report of Two Cases
- PMID: 40524862
- PMCID: PMC12169911
- DOI: 10.70352/scrj.cr.25-0070
Immune Checkpoint Inhibitors for Microsatellite Instability High Unresectable Obstructive Colon Cancer: A Report of Two Cases
Abstract
Introduction: Patients with obstructive colon cancer (OCC) with distant metastases often present with a poor general condition, including malnutrition, anemia, and systemic inflammation. Traditionally, these patients undergo stoma creation and/or primary tumor resection followed by systemic chemotherapy. However, for patients with DNA mismatch repair-deficient/microsatellite instability high (dMMR/MSI-H) colorectal cancer, the emergence of immune checkpoint inhibitors (ICIs) has revolutionized treatment strategies, with remarkable antitumor effects. We report two cases of successful management of MSI-H OCC, achieving curative resection while avoiding decompressive procedures, including colostomy creation.
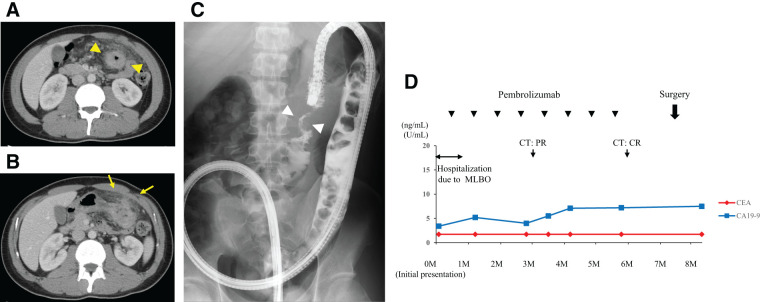
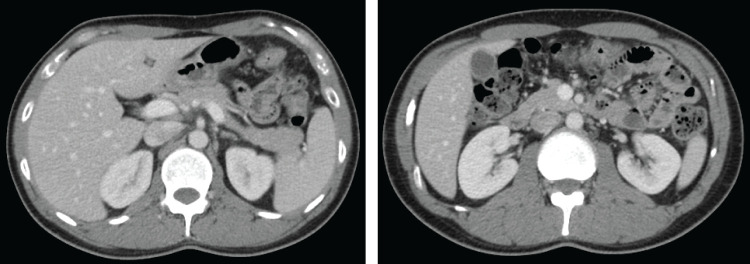
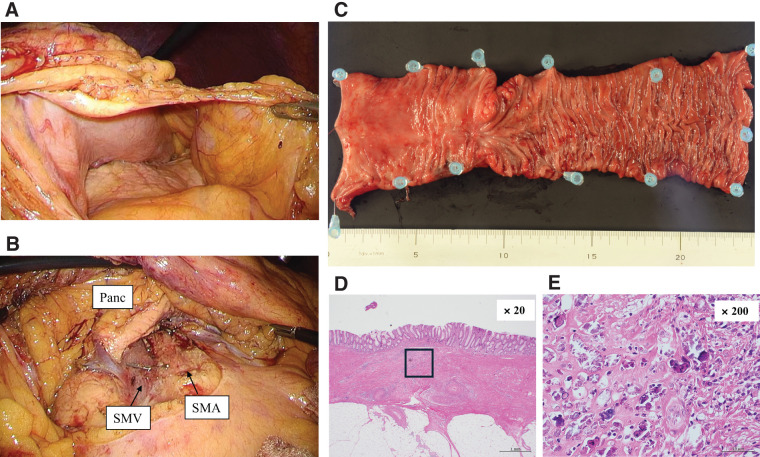
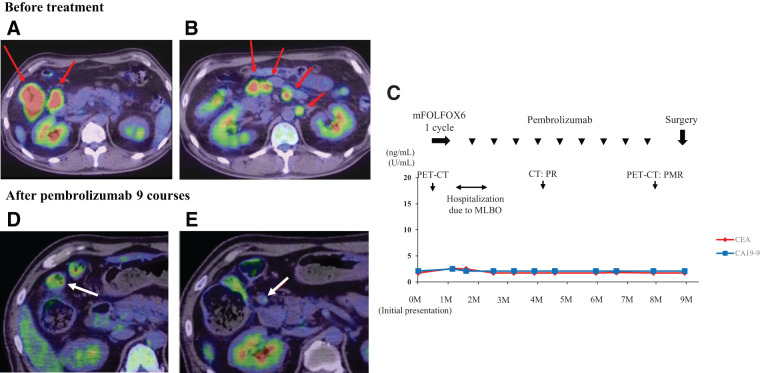
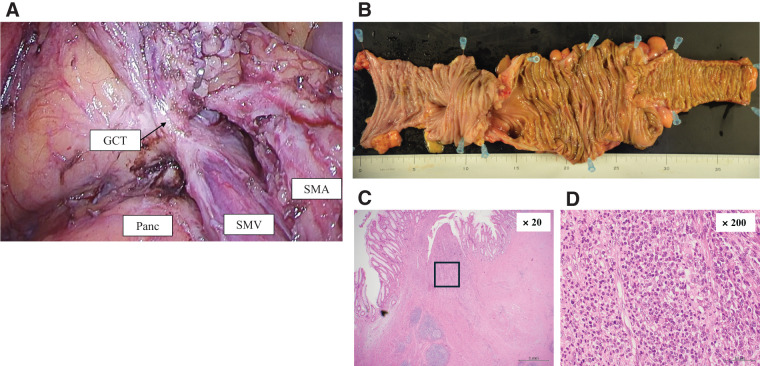
Case presentation: Case 1: A 29-year-old man diagnosed with MSI-H obstructive transverse colon cancer (cT4b stomach, N1b, M1c1) was treated with pembrolizumab monotherapy (200 mg/body, every 3 weeks). The colorectal obstructive scoring system score was 2 at pembrolizumab administration. The patient showed rapid improvement in his abdominal symptoms within 3 days and achieved clinical complete response after eight courses. Laparoscopic partial colectomy with D3 lymph node dissection was subsequently performed safely. He was discharged on postoperative day 8 without postoperative complications. Histopathological analysis confirmed pathological complete response, and the patient was recurrence-free 15 months after surgery without adjuvant chemotherapy. Case 2: A 58-year-old man diagnosed with MSI-H obstructive ascending colon cancer (cT4aN3M1a, LYM) was treated with pembrolizumab monotherapy. The colorectal obstructive scoring system score was 1 at pembrolizumab administration. The patient's abdominal symptoms improved within 5 days, with marked tumor shrinkage after nine courses. Laparoscopic extended right hemi-colectomy with D3 lymph node dissection was subsequently performed safely, and he was discharged on postoperative day 7 without postoperative complications. Histopathological analysis showed major pathological response (less than 10% viable cancer cells in the resected specimen), with no viable tumor cells in the primary lesion. The patient was recurrence-free 1-year post-surgery, without adjuvant chemotherapy.
Conclusions: This report highlights the potential benefits of ICI treatment for dMMR/MSI-H OCC, particularly for rapid relief of obstruction-related symptoms and facilitating oncologically safe R0 resection. In cases of MSI-H OCC, ICIs can be highly effective as an alternative to traditional decompression procedures.
Keywords: MSI-H colorectal cancer; immune checkpoint inhibitors; obstructive colon cancer; pembrolizumab.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Unanticipated pathological clearance in two cases of clinical T4b dMMR/MSI-h advanced colorectal cancer: the potential of immune checkpoint inhibitors despite positive positron-emission tomography results.Surg Case Rep. 2024 May 1;10(1):105. doi: 10.1186/s40792-024-01894-x. Surg Case Rep. 2024. PMID: 38691233 Free PMC article.
-
Conversion surgery for microsatellite instability-high gastric cancer with a complete pathological response to pembrolizumab: a case report.World J Surg Oncol. 2022 Jun 10;20(1):193. doi: 10.1186/s12957-022-02661-8. World J Surg Oncol. 2022. PMID: 35689267 Free PMC article.
-
Pathological Complete Response of Clinical T4b Ascending Colon Cancer after Preoperative Chemotherapy Using Pembrolizumab.Case Rep Oncol. 2021 Oct 19;14(3):1497-1504. doi: 10.1159/000519470. eCollection 2021 Sep-Dec. Case Rep Oncol. 2021. PMID: 34899242 Free PMC article.
-
Neoadjuvant Pembrolizumab Enables Successful Downstaging and Resection of Borderline Resectable MSI-H/dMMR Pancreatic Ductal Adenocarcinoma: A Case Report and Literature Review.J Gastrointest Cancer. 2025 May 8;56(1):112. doi: 10.1007/s12029-025-01237-5. J Gastrointest Cancer. 2025. PMID: 40341577 Free PMC article. Review.
-
Neoadjuvant envafolimab in a patient with MSI-H/dMMR colon cancer: a case report and literature review.Immunotherapy. 2024;16(10):649-657. doi: 10.1080/1750743X.2024.2350355. Epub 2024 May 17. Immunotherapy. 2024. PMID: 39259508 Free PMC article. Review.
References
-
- Yeo HL, Lee SW. Colorectal emergencies: review and controversies in the management of large bowel obstruction. J Gastrointest Surg 2013; 17: 2007–12. - PubMed
-
- Takahashi G, Yamada T, Iwai T, et al. Oncological assessment of stent placement for obstructive colorectal cancer from circulating cell-free DNA and circulating tumor DNA dynamics. Ann Surg Oncol 2018; 25: 737–44. - PubMed