

Creating a Superiorly Based Pharyngeal Flap: Is Prominence of C1 Superior Enough, and Will Adenoid Pad Be in the Way?
- PMID: 40524880
- PMCID: PMC12169972
- DOI: 10.1097/GOX.0000000000006797
Creating a Superiorly Based Pharyngeal Flap: Is Prominence of C1 Superior Enough, and Will Adenoid Pad Be in the Way?
Abstract
Background: Positioning the pharyngeal flap base high along the posterior pharyngeal wall is essential for optimizing speech outcomes. Objective data on where to place the flap base are lacking. Further, adenoid tissue can restrict cephalad positioning of the flap. This study aimed to improve the design of the pharyngeal flap by measuring the distance from the first cervical vertebrae (C1) to the palatal plane, and the adenoid depth in children undergoing evaluation for velopharyngeal insufficiency.
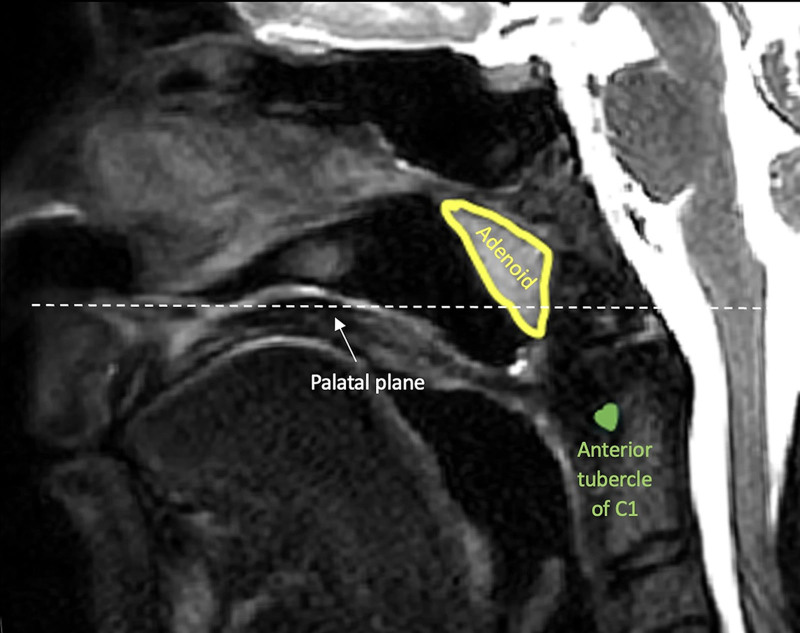
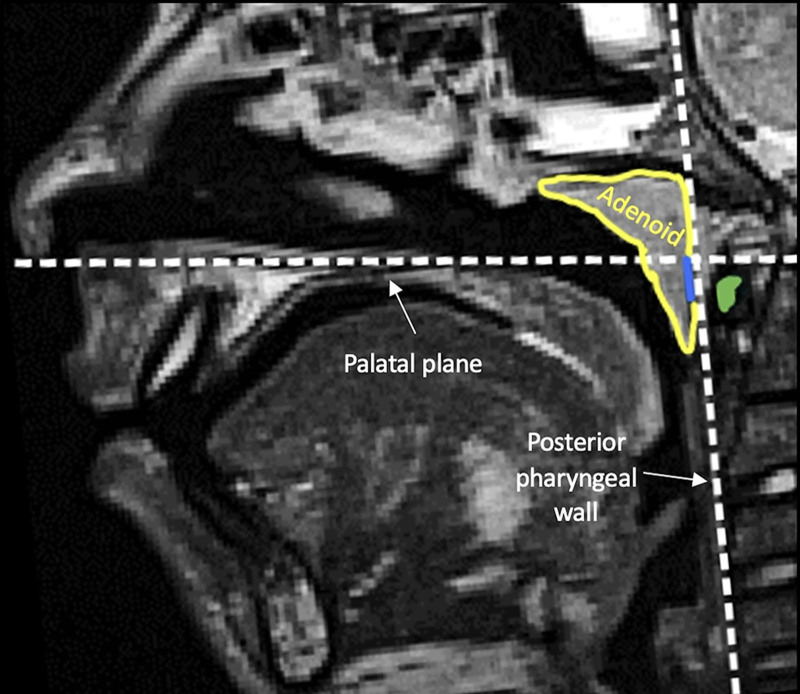
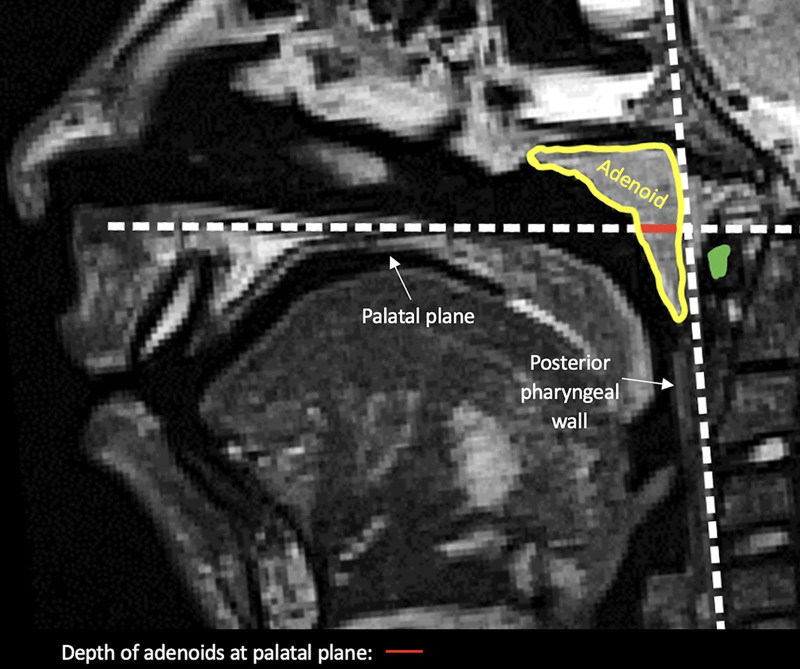
Methods: This retrospective cross-sectional study analyzed magnetic resonance imaging (MRI) scans of the velopharynx and measured the distance between C1 and the palatal plane, and the adenoid depth at the level of the palatal plane in millimeters.
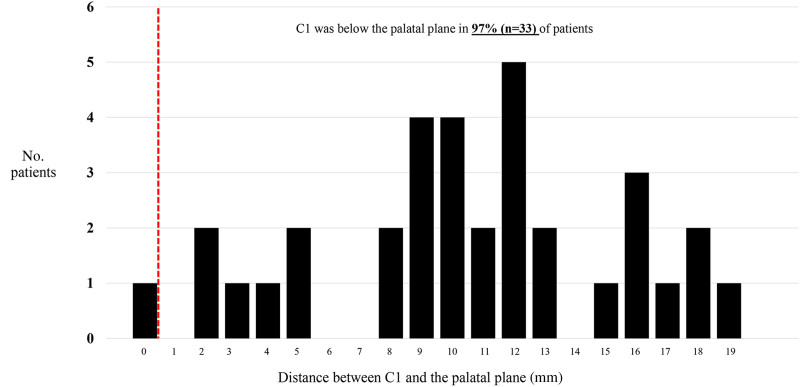
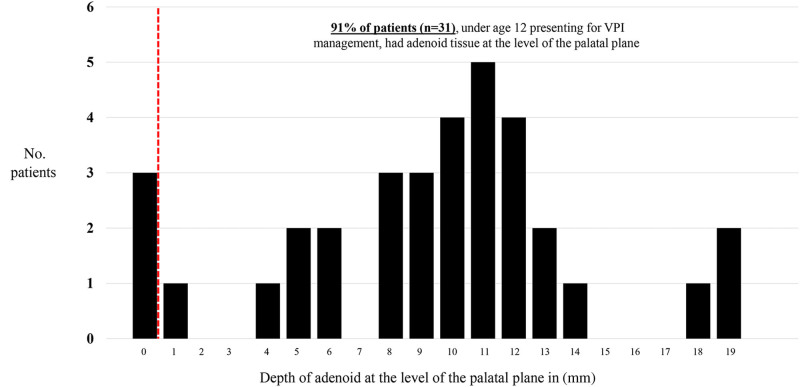
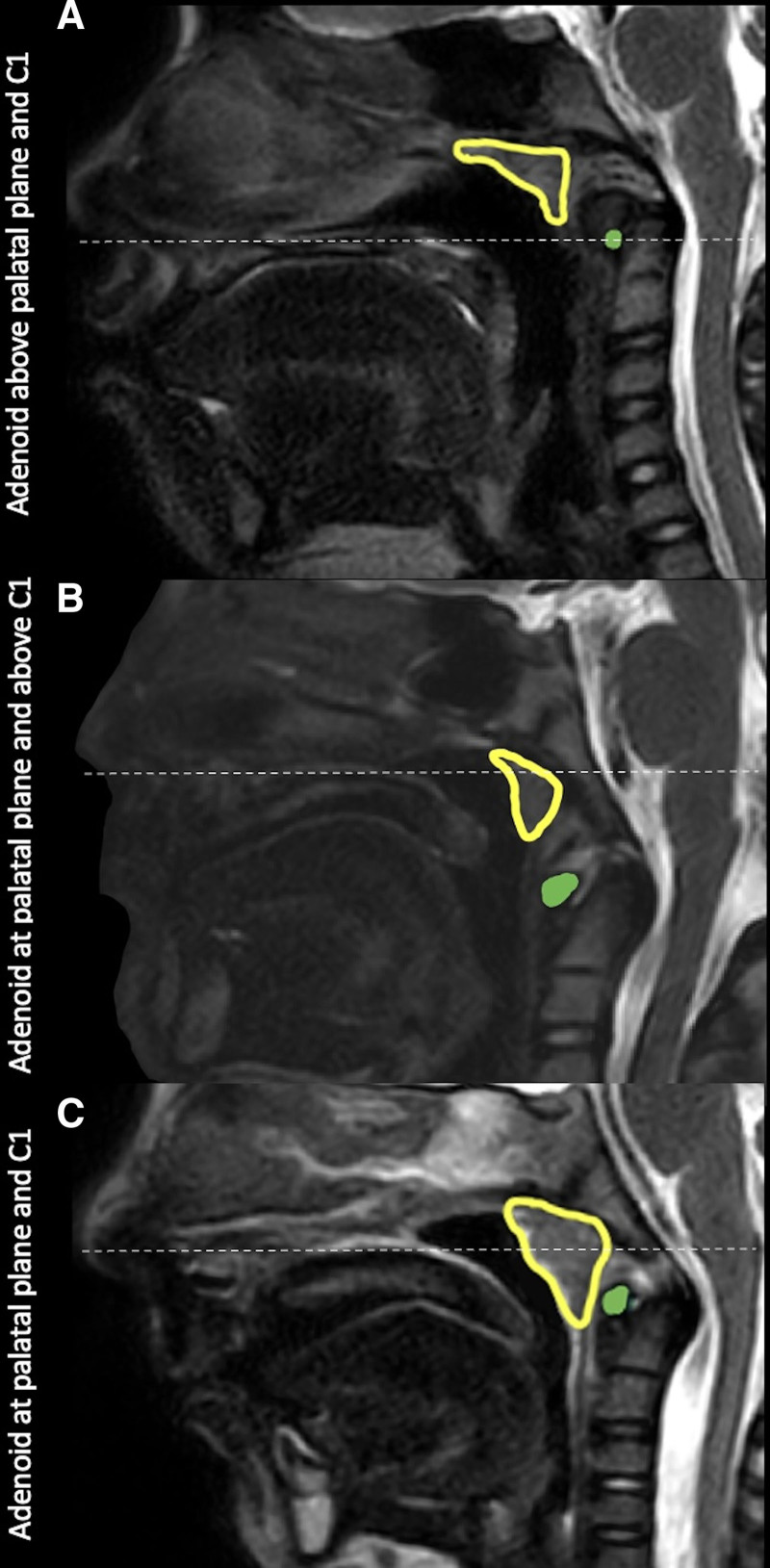
Results: Thirty-four patients met the inclusion criteria. The mean age at the time of MRI was 7.4 years (range: 3.9-11.9 y). The anterior tubercle of C1 was below the palatal plane in 97% (n = 33) of patients. On average, this landmark was 10.5 mm (SD = 5.0) below the palatal plane. Adenoid tissue was present at the level of the palatal plane in 91% (n = 31) of patients.
Conclusions: Positioning the pharyngeal flap base at C1 is too low to aid with velopharyngeal closure. Further, adenoid tissue is frequently present at the level of velopharyngeal closure, limiting superior positioning of the pharyngeal flap base. When this occurs, surgeons should consider adenoidectomy before pharyngeal flap surgery. Preoperative MRI may be beneficial for planning pharyngeal flap positioning relative to C1 and assessing adenoid tissue at the palatal plane.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article. Research reported in this publication was supported by the National Institute of Dental and Craniofacial Research of the National Institutes of Health under Award Numbers F31DE033236, K23DE025023, and U01DE029750. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Figures
References
-
- Kummer AW, Clark SL, Redle EE, et al. Current practice in assessing and reporting speech outcomes of cleft palate and velopharyngeal surgery: a survey of cleft palate/craniofacial professionals. Cleft Palate Craniofac J. 2012;49:146–152. - PubMed
-
- Willging JP. Superiorly based pharyngeal flap and posterior pharyngeal wall augmentation. Oper Tech Otolaryngol Head Neck Surg. 2009;20:268–273.
-
- Emara TA, Quriba AS. Posterior pharyngeal flap for velopharyngeal insufficiency patients: a new technique for flap inset. Laryngoscope. 2012;122:260–265. - PubMed
-
- Sitzman TJ, Williams JL, Singh DJ, et al. Magnetic resonance imaging of the velopharynx: clinical findings in patients with velopharyngeal insufficiency. Plast Reconstr Surg. 2024;153:1155e–1168e. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous