

Energy doses for paediatric defibrillation in cardiac arrest: systematic review and meta-analysis
- PMID: 40524976
- PMCID: PMC12169708
- DOI: 10.1016/j.resplu.2025.100991
Energy doses for paediatric defibrillation in cardiac arrest: systematic review and meta-analysis
Abstract
Background: Early defibrillation is the foundation of treatment of shockable ventricular arrhythmias (VF, pVT) but optimal energy doses for initial and subsequent shocks in paediatric cardiac arrest remain controversial.
Objectives: To assess the use of different energy doses for initial defibrillation in infants, children and adolescents with ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT) during cardiac arrest.
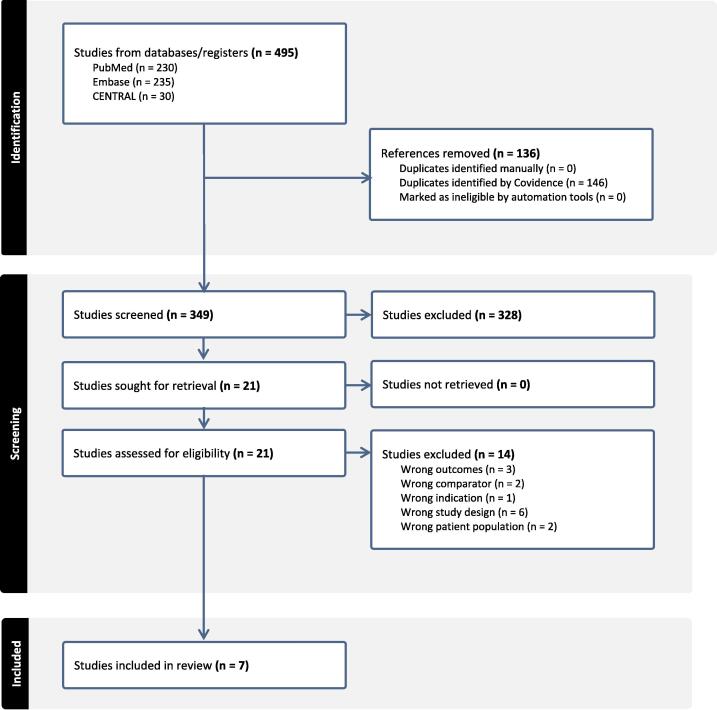
Methods: A systematic review was performed by the ILCOR Paediatric Life Support Task force. This systematic review was prospectively registered as PROSPERO CRD42024548898. A search of PubMed, EMBASE, and Cochrane Controlled Register of Trials (CENTRAL) was performed for clinical trials and observational studies, published before 1 January 2025, involving cardiac defibrillation in infants and children (excluding newborn infants) in cardiac arrest. Investigators reviewed studies for relevance, extracted data, and assessed risk of bias using the ROBINS-I framework. Critical outcomes included survival to hospital discharge and return of spontaneous circulation. Results were compiled into a Summary of Findings table using the GRADEpro Guideline Development tool. Statistical calculations and Forest plot generation were performed using RevMan.
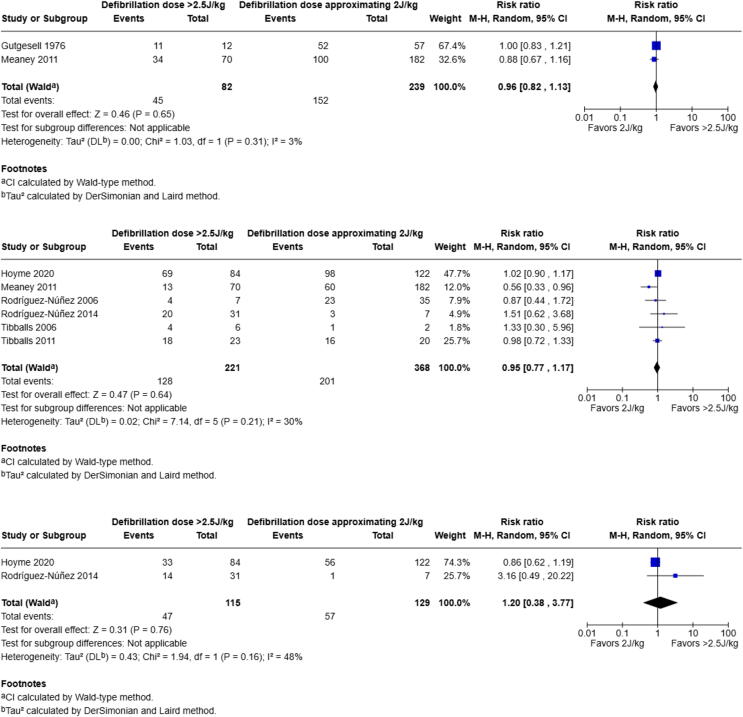
Results: We identified 7 relevant observational studies. The majority of studies involved in-hospital cardiac arrest. The overall certainty of evidence was very low. Critical (survival to hospital discharge, return of spontaneous circulation) and important (termination of VF/pVT) outcomes were not significantly better or worse when initial defibrillation doses of <1.5 J/kg or >2.5 J/kg were used for children in cardiac arrest with a shockable rhythm compared with initial doses approximating 2 J/kg.
Conclusions: The current available data suggest that outcomes are not significantly better or worse when initial defibrillation doses of <1.5 J/kg or >2.5 J/kg are used for children in cardiac arrest with a shockable rhythm (VF or pVT) compared with initial doses approximating 2 J/kg. Well-designed randomised trials are needed to address this important question.
Keywords: Cardiac arrest; Cardioversion; Defibrillation; Dose; Paediatric.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. Monica Kleinman serves on the Editorial Board of the Resuscitation Journal. She was not involved in the editorial review or the decision to publish this article.
Figures

References
-
- Van de Voorde P., Turner N.M., Djakow J., et al. European Resuscitation Council Guidelines 2021: paediatric life support. Resuscitation. 2021;161:327–387. - PubMed
-
- ANZCOR. Guideline 12.2 – Paediatric Advanced Life Support (PALS); 2021. Available at: https://www.anzcor.org/home/paediatric-advanced-life-support/guideline-1....
-
- Topjian A.A., Raymond T.T., Atkins D., et al. Part 4: pediatric basic and advanced life support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142:S469–S523. - PubMed
-
- Mercier E., Laroche E., Beck B., et al. Defibrillation energy dose during pediatric cardiac arrest: systematic review of human and animal model studies. Resuscitation. 2019;139:241–252. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
