

Minimally Invasive vs Conventional Coronary Bypass Surgery for Multivessel Coronary Disease
- PMID: 40525194
- PMCID: PMC12167539
- DOI: 10.1016/j.atssr.2024.10.024
Minimally Invasive vs Conventional Coronary Bypass Surgery for Multivessel Coronary Disease
Abstract
Background: Despite sternum sparing and without cardiopulmonary bypass, the actual value of minimally invasive coronary surgery (MICS) is still debatable. This study aimed to compare the completeness of revascularization and intermediate-term outcomes of MICS with conventional sternotomy coronary artery bypass grafting (CABG).
Methods: Two groups of 244 patients each receiving MICS-CABG and sternotomy-CABG between November 2015 and March 2019 were matched by propensity score matching. The completeness of revascularization and major adverse cardiovascular and cerebrovascular events (MACCE; a composite of death, myocardial infarction, stroke, or repeated target vessel revascularization) were compared between the groups.
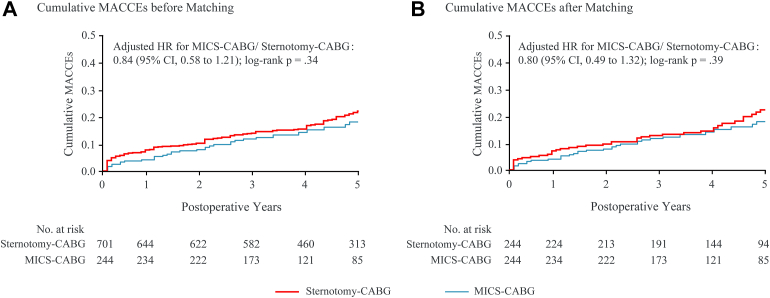
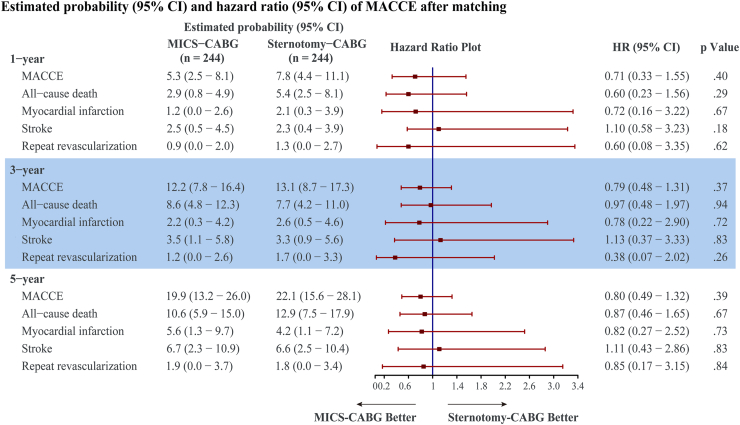
Results: In the MICS-CABG group, the percentages of bypassed vessels 2, 3, and ≥4 were 53.7%, 36.1%, and 10.2%, respectively. Completeness of revascularization (95.5% vs 96.3%; P = .65) was comparable between MICS-CABG and sternotomy-CABG groups. Postprocedural angiography revealed an overall patency of 96.2% (578/601) for the MICS-CABG group. At 5 years, rates of MACCE (19.9% vs 22.1%; hazard ratio [HR], 0.80; 95% CI, 0.49-1.32; P = .39), death (10.6% vs 12.9%; HR, 0.87; 95% CI, 0.46-1.65; P = .67), myocardial infarction (5.6% vs 4.2%; HR, 0.82; 95% CI, 0.27-2.52; P = .73), stroke (6.7% vs 6.6%; HR, 1.11; 95% CI, 0.43-2.86; P = .83), and repeated target vessel revascularization (1.9% vs 1.8%; HR, 0.85; 95% CI, 0.17-3.15; P = .84) were similar between MICS-CABG and sternotomy-CABG.
Conclusions: MICS-CABG, which appeared to yield noninferior completeness of revascularization and intermediate-term MACCE compared with sternotomy-CABG, could be an alternative for patients with multivessel coronary diseases.
© 2024 The Authors.
Figures



Similar articles
-
Comparing patient outcomes following minimally invasive coronary artery bypass grafting surgery vs. coronary artery bypass grafting: a single-center retrospective cohort study.Cardiovasc Diagn Ther. 2022 Jun;12(3):378-388. doi: 10.21037/cdt-22-10. Cardiovasc Diagn Ther. 2022. PMID: 35800361 Free PMC article.
-
Hybrid total arterial minimally invasive off-pump coronary revascularization and percutaneous coronary intervention strategy for multivessel coronary artery disease: a cohort study with a median 11-year follow-up.Cardiovasc Diagn Ther. 2024 Apr 30;14(2):272-282. doi: 10.21037/cdt-23-413. Epub 2024 Apr 18. Cardiovasc Diagn Ther. 2024. PMID: 38716312 Free PMC article.
-
The efficacy of minimally invasive coronary artery bypass grafting (mics cabg) for patients with coronary artery diseases and diabetes: a single center retrospective study.J Cardiothorac Surg. 2024 Apr 18;19(1):244. doi: 10.1186/s13019-024-02717-8. J Cardiothorac Surg. 2024. PMID: 38632609 Free PMC article.
-
Less invasive multivessel coronary artery bypass grafting: now is the time.Curr Opin Cardiol. 2021 Nov 1;36(6):735-739. doi: 10.1097/HCO.0000000000000906. Curr Opin Cardiol. 2021. PMID: 34456253 Review.
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
Cited by
-
Minimally invasive coronary bypass grafting for treating multivessel coronary disease: A single-center prospective pilot study.JTCVS Open. 2025 May 4;25:96-119. doi: 10.1016/j.xjon.2025.03.030. eCollection 2025 Jun. JTCVS Open. 2025. PMID: 40631015 Free PMC article.
-
Dietary modulation of pubertal timing: gut microbiota-derived SCFAs and neurotransmitters orchestrate hypothalamic maturation via the gut-brain axis.J Endocrinol Invest. 2025 Jun 17. doi: 10.1007/s40618-025-02615-3. Online ahead of print. J Endocrinol Invest. 2025. PMID: 40526265 Review.
References
-
- Thuijs D., Kappetein A.P., Serruys P.W., et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. Lancet. 2019;394:1325–1334. doi: 10.1016/s0140-6736(19)31997-x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
