

Bystander CPR Technique and Outcomes for Cardiac Arrest With and Without Opioid Toxicity
- PMID: 40526383
- PMCID: PMC12175020
- DOI: 10.1001/jamanetworkopen.2025.16340
Bystander CPR Technique and Outcomes for Cardiac Arrest With and Without Opioid Toxicity
Abstract
Importance: Previous studies support bystander provision of chest compression-only cardiopulmonary resuscitation (CC-CPR) for out-of-hospital cardiac arrest (OHCA). However, it is unknown whether OHCA secondary to opioid toxicity may benefit from chest compression plus ventilation CPR (CCV-CPR).
Objective: To examine the association between bystander CPR technique and outcomes among both opioid-associated OHCA (OA-OHCA) and otherwise undifferentiated OHCA.
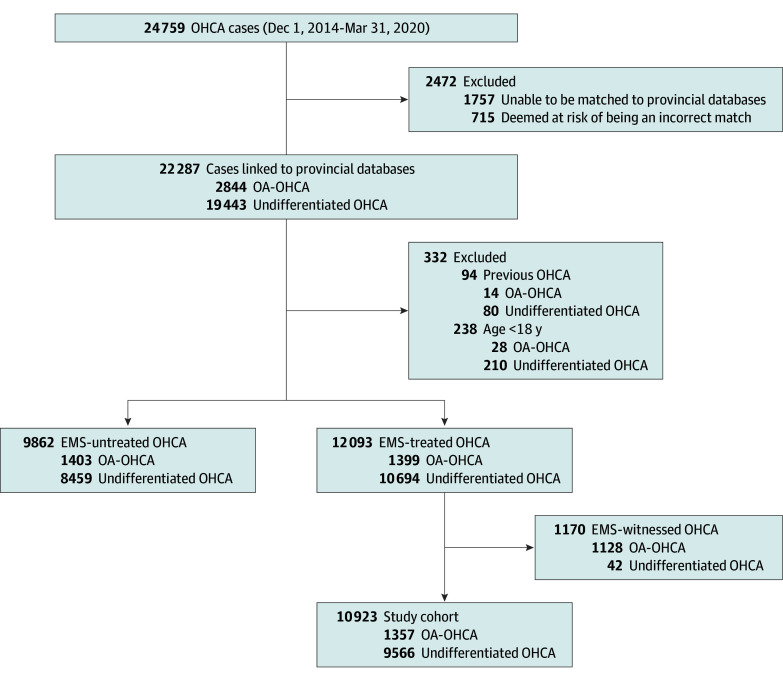
Design, setting, and participants: This cohort study (performed from August 1, 2023, to December 31, 2024) analyzed cases of adult emergency medical services-treated OHCA that occurred from December 1, 2014, to March 31, 2020, as identified through the British Columbia Cardiac Arrest Registry.
Exposures: Cases were classified as OA-OHCA based on positive postmortem toxicologic investigations, death certificates, or opioid-specific hospital-based diagnoses. All other cases were classified as undifferentiated OHCA.
Main outcomes and measures: Favorable neurologic outcome at hospital discharge (cerebral performance category ≤2). A multivariable Utstein-adjusted logistic regression model of complete cases was used to assess the association between bystander CPR technique (CC-CPR [reference] vs both CCV-CPR and no CPR individually) with outcomes. An interaction term between the OA-OHCA and bystander CPR technique was used to estimate associations among OA-OHCA and undifferentiated OHCA cases separately.
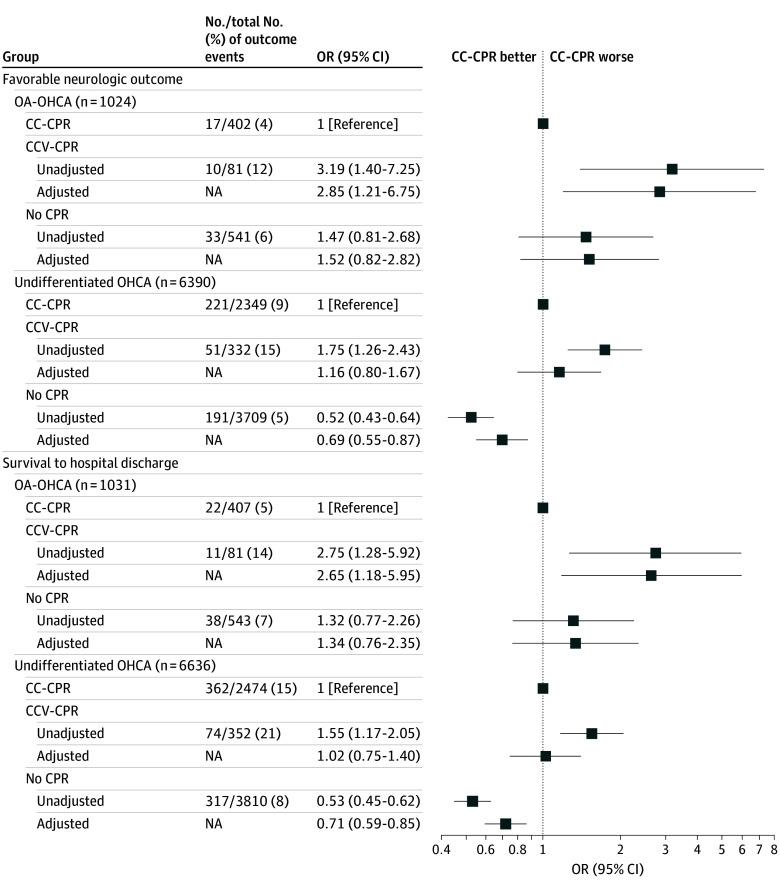
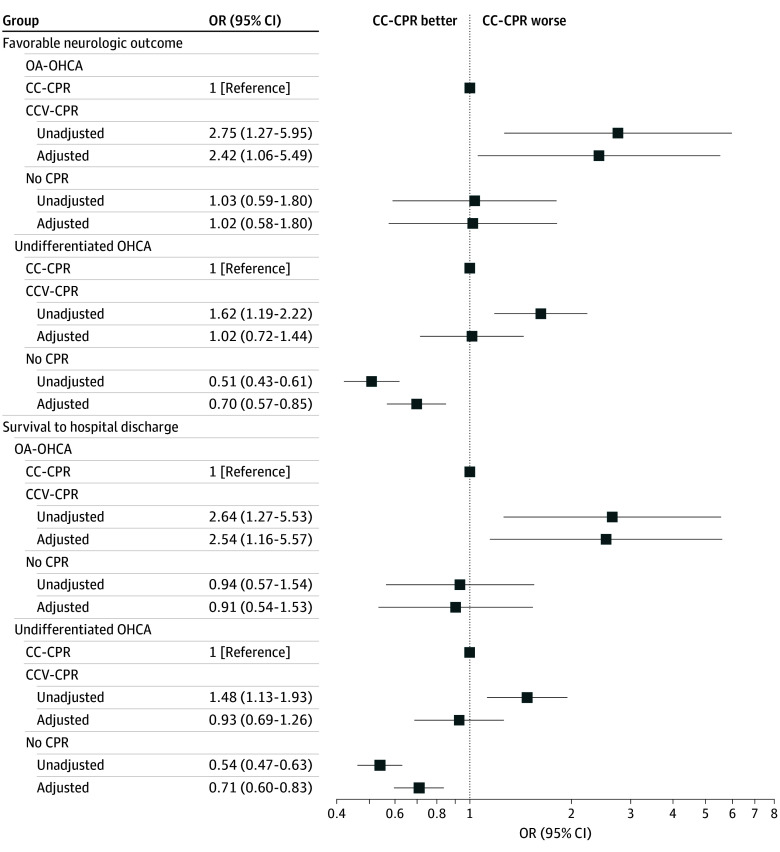
Results: The study included 10 923 OHCAs. After removing 24 cases only treated with ventilatory support, there were 1343 OA-OHCAs (median [IQR] patient age, 40 [31-50] years; 1015 [76%] male) and 9556 undifferentiated OHCAs (median [IQR] patient age, 70 [58-81] years; 6636 (69%) male). In the OA-OHCA group, bystander CCV-CPR was associated with an increased odds of a favorable neurologic outcome (adjusted odds ratio [AOR], 2.85; 95% CI, 1.21-6.75) when compared with CC-CPR. No association was detected with favorable neurologic outcome (AOR, 1.52; 95% CI, 0.82-2.82) when no CPR was compared with CC-CPR. Among undifferentiated OHCAs, no association was detected with a favorable neurologic outcome (AOR, 1.16; 95% CI, 0.80-1.67) when CCV-CPR was compared with CC-CPR. No CPR was associated with a decreased odds of a favorable neurologic outcome (AOR, 0.69; 95% CI, 0.55-0.87) when compared with CC-CPR. The interaction term was statistically significant (P for interaction = .04).
Conclusions and relevance: In this cohort study of OHCA, bystander CCV-CPR (compared with CC-CPR) was associated with improved outcomes in opioid-associated OHCA; however, this association was not observed among undifferentiated cardiac arrests. These results suggest that the optimal bystander CPR technique for OA-OHCA and undifferentiated OHCA may differ and that ventilations may improve outcomes in OA-OHCA resuscitation.
Conflict of interest statement
Figures
Comment in
- doi: 10.1001/jamanetworkopen.2025.16348
Similar articles
-
Resuscitation Attempt and Outcomes in Patients With Asystole Out-of-Hospital Cardiac Arrest.JAMA Netw Open. 2024 Nov 4;7(11):e2445543. doi: 10.1001/jamanetworkopen.2024.45543. JAMA Netw Open. 2024. PMID: 39556393 Free PMC article.
-
Rurality and Area Deprivation and Outcomes After Out-of-Hospital Cardiac Arrest.JAMA Netw Open. 2025 Apr 1;8(4):e253435. doi: 10.1001/jamanetworkopen.2025.3435. JAMA Netw Open. 2025. PMID: 40232722 Free PMC article.
-
Association between time taken to start dispatch assisted-bystander cardiopulmonary resuscitation (DA-CPR) and outcomes for out-of-hospital cardiac arrest (OHCA).Resuscitation. 2025 Aug;213:110651. doi: 10.1016/j.resuscitation.2025.110651. Epub 2025 May 21. Resuscitation. 2025. PMID: 40409669
-
In patients with out-of-hospital cardiac arrest, does the provision of dispatch cardiopulmonary resuscitation instructions as opposed to no instructions improve outcome: a systematic review of the literature.Resuscitation. 2011 Dec;82(12):1490-5. doi: 10.1016/j.resuscitation.2011.09.004. Epub 2011 Sep 16. Resuscitation. 2011. PMID: 21925129
-
Effectiveness of different compression-to-ventilation methods for cardiopulmonary resuscitation: A systematic review.Resuscitation. 2017 Sep;118:112-125. doi: 10.1016/j.resuscitation.2017.05.032. Epub 2017 Jun 2. Resuscitation. 2017. PMID: 28583860
References
-
- Standing Committee on Health Studies Report. Report and recommendations on the opioid crisis in Canada. 2015. Accessed December 1, 2024. https://www.ourcommons.ca/documentviewer/en/42-1/HESA/report-6/page-66#recs
-
- BC Ministry of Health . Provincial health officer declares public health emergency. April 2016. Accessed December 1, 2024. https://news.gov.bc.ca/releases/2016HLTH0026-000568
-
- Becerra X. Renewal of determination that a public health emergency exists. Administration for Strategic Preparedness and Response. September 2024. Accessed December 1, 2024. https://aspr.hhs.gov/legal/PHE/Pages/Opioid-September2024-aspx.aspx
-
- Spencer M, Garnett M, Miniño A.. Drug Overdose Deaths in the United States, 2002-2022. NCHS Data Brief No. 491. March 2024. Accessed April 28, 2025. https://www.cdc.gov/nchs/products/databriefs/db491.htm
-
- Public Health Agency of Canada . Federal, provincial, and territorial Special Advisory Committee on Toxic Drug Poisonings. September 2024. Accessed November 5, 2024. https://health-infobase.canada.ca/substance-related-harms/opioids-stimul...
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
