

Safety Evaluation in Healthy Adults of Motion-Based Virtual Reality Dichoptic Training for Pediatric Patients With Amblyopia: Prospective Intervention Study
- PMID: 40526901
- PMCID: PMC12187024
- DOI: 10.2196/69801
Safety Evaluation in Healthy Adults of Motion-Based Virtual Reality Dichoptic Training for Pediatric Patients With Amblyopia: Prospective Intervention Study
Abstract
Background: Amblyopia, a unilateral or bilateral visual disorder, affects up to 5% of the general population and is a leading cause of childhood visual impairment. Current treatments, such as patching therapy, aim to improve amblyopia by temporarily occluding the unaffected eye, thereby promoting the use of the amblyopic eye. However, adherence to patch therapy can be challenging, as the forced use of the amblyopic eye can be stressful for children. Moreover, despite improvements in visual acuity by patch therapy, children with amblyopia often face difficulties with hand-eye coordination; therefore, a treatment that reduces stress for them while simultaneously improving hand-eye coordination could address the limitations of existing amblyopia therapies.
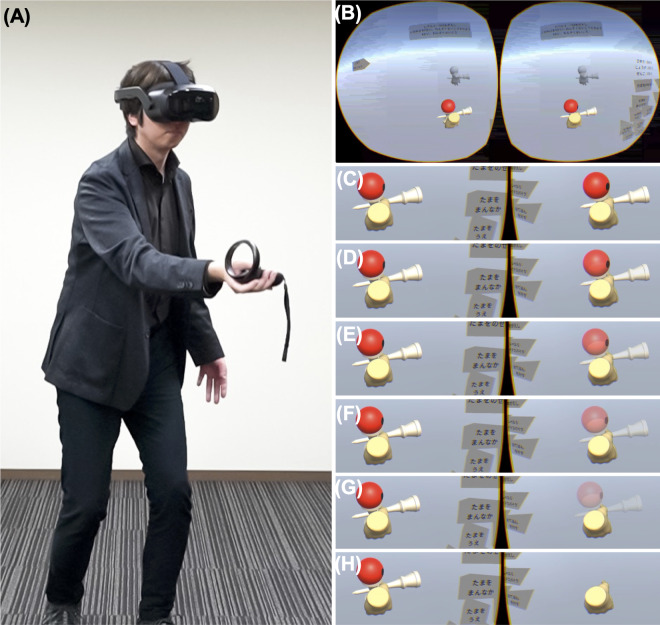
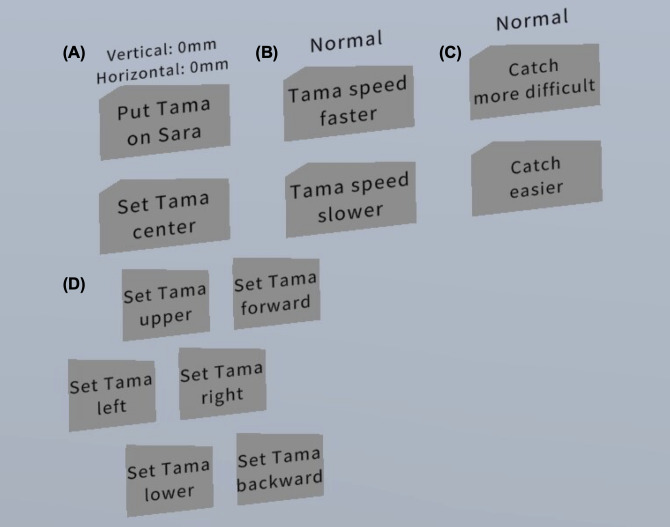
Objective: This study investigated the safety of our motion-based virtual reality (VR) dichoptic training app using Japanese Kendama in healthy adult participants, which was designed to improve hand-eye coordination in pediatric patients with amblyopia.
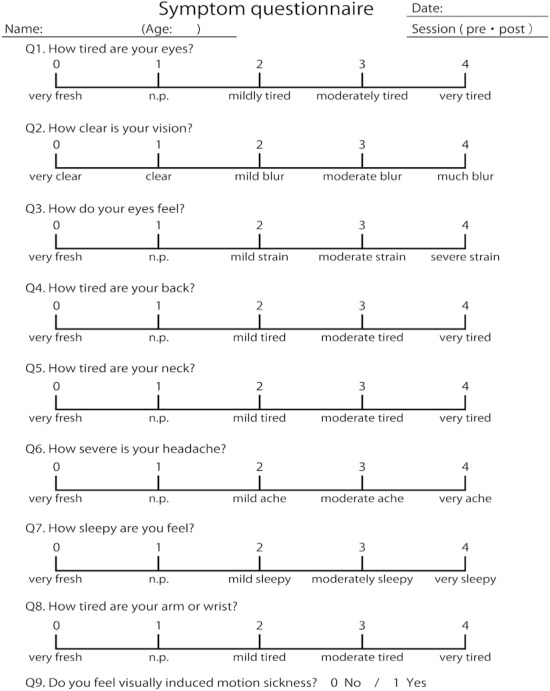
Methods: This prospective intervention study involved 20 healthy young adults (median age 21, IQR 21-28.3 y), including 16 women. The participants played the motion-based VR dichoptic training app for 30 minutes and then completed a subjective symptom questionnaire, which comprised 9 questions (Q1-Q9) with each item scored on a 4-point scale, except Q9, which was assessed on a binary scale. Q1-Q3 focused on subjective eye symptoms, Q4-Q7 evaluated physical and mental discomfort, Q8 assessed the degree of VR session-induced arm fatigue, and Q9 assessed the severity of visually induced motion sickness.
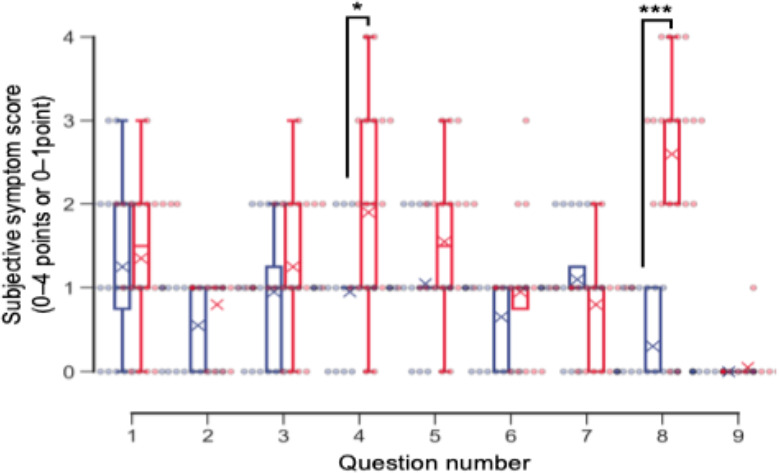
Results: No significant differences were observed in the reported ocular symptoms before and after the VR session, including eye fatigue (mean before vs after: 1.25, SD 0.94 points vs 1.35, SD 0.85 points), blurred vision (0.55, SD 0.50 points vs 0.80, SD 0.40 points), eye dryness (0.95, SD 0.74 points vs 1.25, SD 0.83 points), and visually induced motion sickness (0.00, SD 0.00 points vs 0.05, SD 0.22 points). These results suggested that the motion-based VR dichoptic training did not induce significant adverse ocular effects.
Conclusions: The motion-based VR dichoptic training app demonstrated minimal adverse ocular effects in healthy adult participants, suggesting that it is safe for use in this population. These findings demonstrate the feasibility and good tolerability of this VR-based intervention in healthy adults. Further studies, including clinical studies in adult and pediatric patients with amblyopia, are warranted to evaluate its applicability and therapeutic effects.
Keywords: adherence; amblyopia; dichoptic training; digital health; digital therapeutics; safety evaluation; strabismus; virtual reality; visually induced motion sickness.
© Masakazu Hirota, Yuichi Okumura, Ken Nagino, Takao Hayashi, Takashi Negishi, Shintaro Nakao, Hitoshi Kawasaki, Takenori Inomata. Originally published in JMIR Formative Research (https://formative.jmir.org).
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
