

Comparisons of mortality predictions of mROX, CURB-65, and APACHE II in patients with severe pneumonia: A retrospective cohort study
- PMID: 40527785
- PMCID: PMC12173283
- DOI: 10.1097/MD.0000000000042931
Comparisons of mortality predictions of mROX, CURB-65, and APACHE II in patients with severe pneumonia: A retrospective cohort study
Abstract
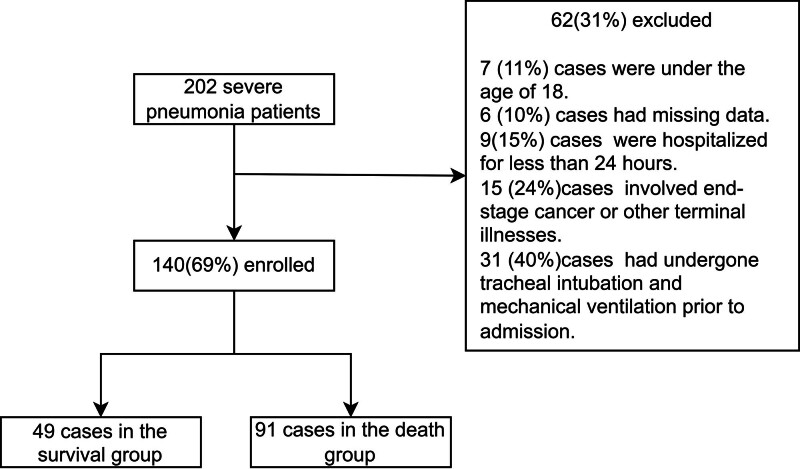
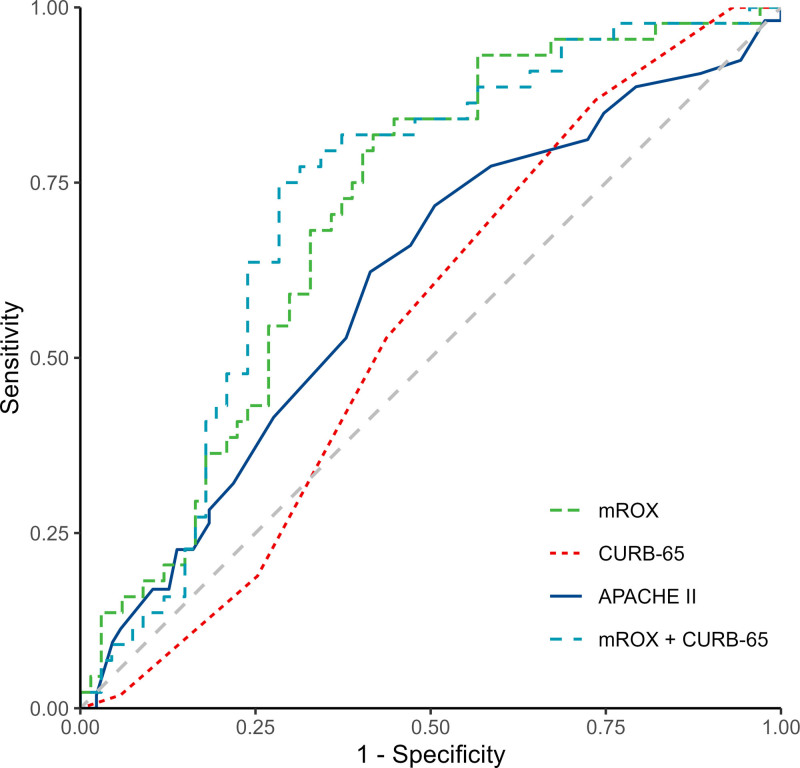
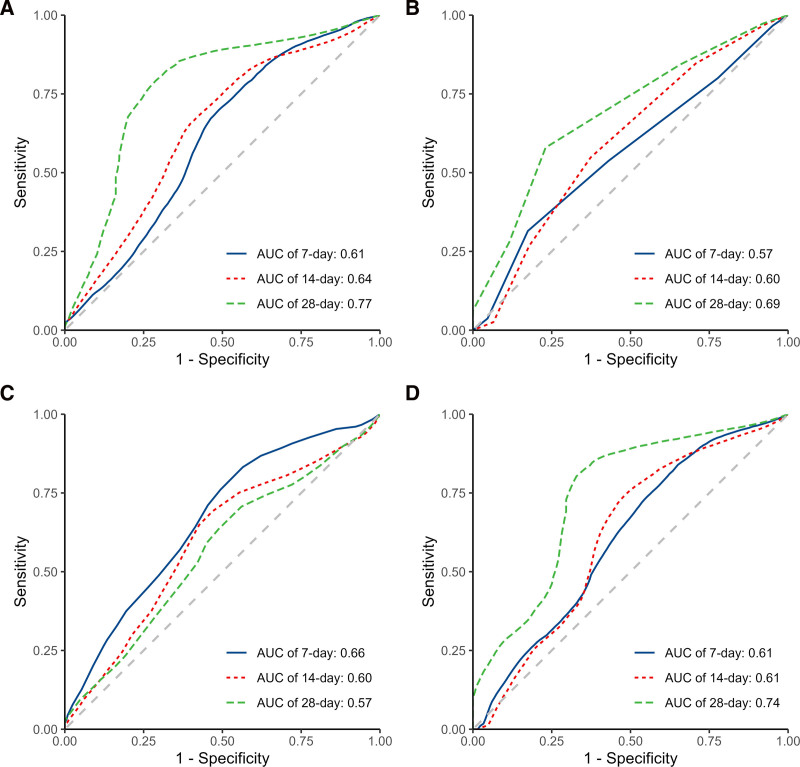
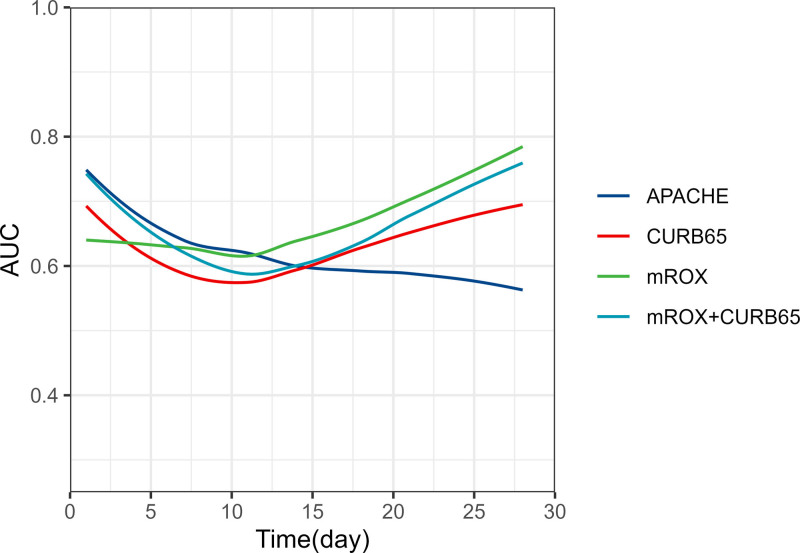
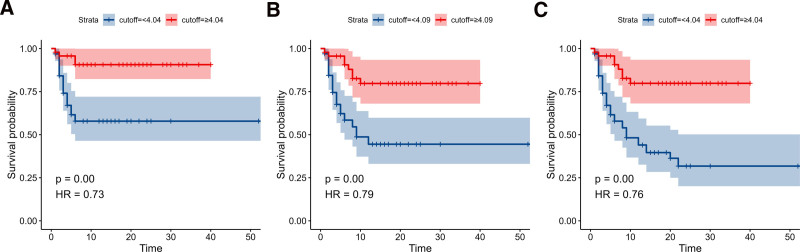
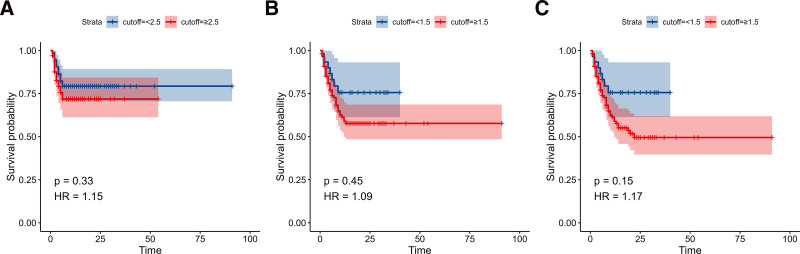
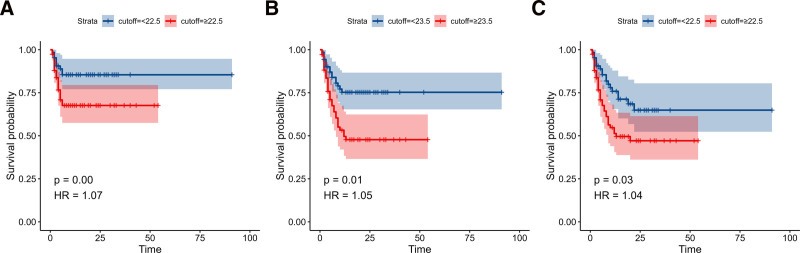
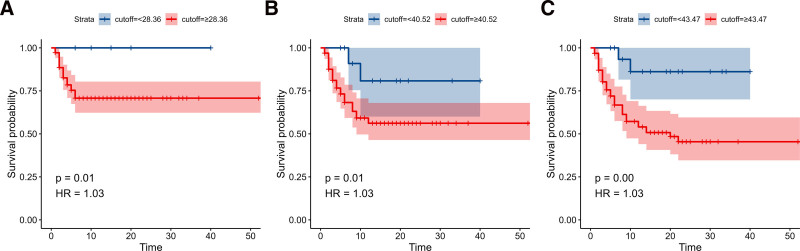
This study investigates the efficacy of the modified respiratory rate oxygenation (mROX) index, the CURB-65 score, their combination, and the Acute Physiology and Chronic Health Evaluation (APACHE) II score in predicting mortality among patients with severe pneumonia over various time frames. This retrospective cohort study analyzed data from patients admitted with severe pneumonia between January 2017 and December 2023. Patient demographics and 7-, 14-, and 28-day mortality outcomes were collected. The mROX, CURB-65, and APACHE II scores were computed upon hospital admission. The receiver operating characteristic (ROC) curve, time-dependent ROC curve, and survival curve analyses were conducted to assess the mortality predictive performance of mROX, CURB-65, and their combination, as well as APACHE II. The study included 140 patients, of whom 100 (71.4%) were male, with a median age of 65.0 years (interquartile range: 24.0). Within 28 days, 91 (65.0%) patients had succumbed. Compared to survivors, deceased patients exhibited higher CURB-65 scores and lower mROX indices. ROC analysis indicated that mROX outperformed CURB-65 and APACHE II in sensitivity, accuracy, and area under the curve (AUC) for predicting 28-day mortality. The combination of mROX and CURB-65 yielded the highest AUC (72.1%), suggesting enhanced mortality prediction accuracy. Time-dependent ROC and AUC analyses demonstrated the superior predictive capability of APACHE II within the initial 7 days post-admission, while mROX and CURB-65, alone or combined, were more effective for predictions beyond 14 days. Kaplan-Meier survival analysis indicated that higher mROX values and lower scores of CURB-65 and the combination of both were associated with reduced mortality risk, whereas APACHE II showed no significant difference in mortality risk. The mROX index, particularly when combined with CURB-65, improves mortality prediction accuracy in severe pneumonia patients beyond 14 days post-admission. The APACHE II score remains a valuable predictor within the first 7 days.
Keywords: Acute Physiology and Chronic Health Evaluation; CURB-65; modified respiratory rate oxygenation index; mortality; prediction model; severe pneumonia.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Machine learning-based model for predicting all-cause mortality in severe pneumonia.BMJ Open Respir Res. 2025 Mar 22;12(1):e001983. doi: 10.1136/bmjresp-2023-001983. BMJ Open Respir Res. 2025. PMID: 40122535 Free PMC article.
-
Predictive value of mNUTRIC score for chronic critical illness in patients of sepsis complicated with ARDS.Technol Health Care. 2025 Mar;33(2):831-837. doi: 10.1177/09287329241296430. Epub 2024 Nov 15. Technol Health Care. 2025. PMID: 39973838
-
Rectus femoris and vastus intermedius muscle thickness as a predictor of mortality in elderly patients with pneumonia.Am J Emerg Med. 2025 Sep;95:200-208. doi: 10.1016/j.ajem.2025.06.065. Epub 2025 Jun 26. Am J Emerg Med. 2025. PMID: 40596798
-
Value of severity scales in predicting mortality from community-acquired pneumonia: systematic review and meta-analysis.Thorax. 2010 Oct;65(10):884-90. doi: 10.1136/thx.2009.134072. Epub 2010 Aug 20. Thorax. 2010. PMID: 20729235
-
Risk prediction models for mortality in patients with ventilator-associated pneumonia: A systematic review and meta-analysis.J Crit Care. 2017 Feb;37:112-118. doi: 10.1016/j.jcrc.2016.09.003. Epub 2016 Sep 13. J Crit Care. 2017. PMID: 27676171
References
-
- Calabretta D, Martìn-Loeches I, Torres A. New guidelines for severe community-acquired pneumonia. Semin Respir Crit Care Med. 2024;45:274–86. - PubMed
-
- Cillóniz C, Torres A, Niederman MS. Management of pneumonia in critically ill patients. BMJ. 2021;375:e065871. - PubMed
-
- Mortensen EM, Restrepo M, Anzueto A, Pugh J. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med. 2004;117:726–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
