

Total cholesterol/high-density lipoprotein cholesterol-related indices as predictors of obstructive sleep apnea and cardiovascular mortality: A cross-sectional study
- PMID: 40527802
- PMCID: PMC12173314
- DOI: 10.1097/MD.0000000000042872
Total cholesterol/high-density lipoprotein cholesterol-related indices as predictors of obstructive sleep apnea and cardiovascular mortality: A cross-sectional study
Abstract
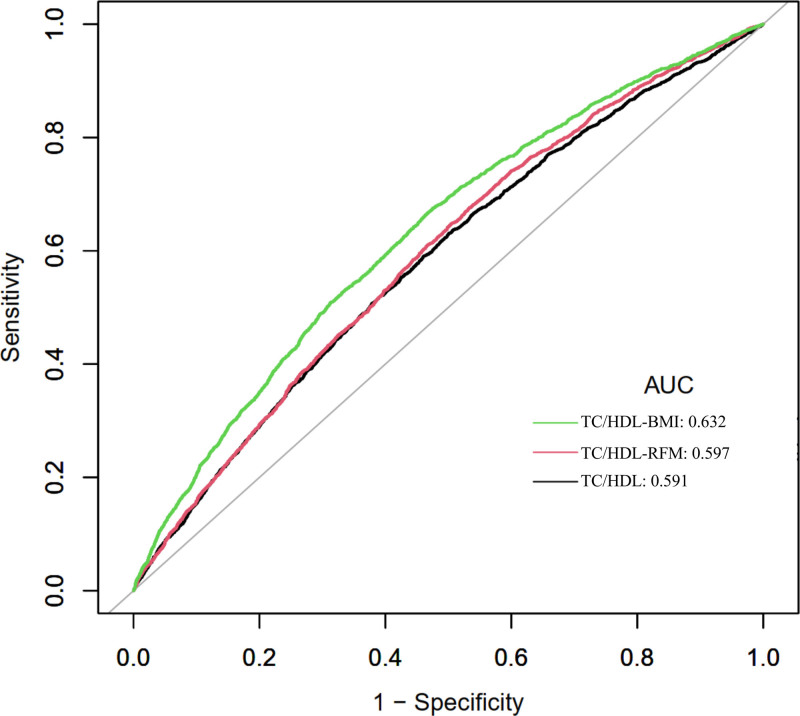
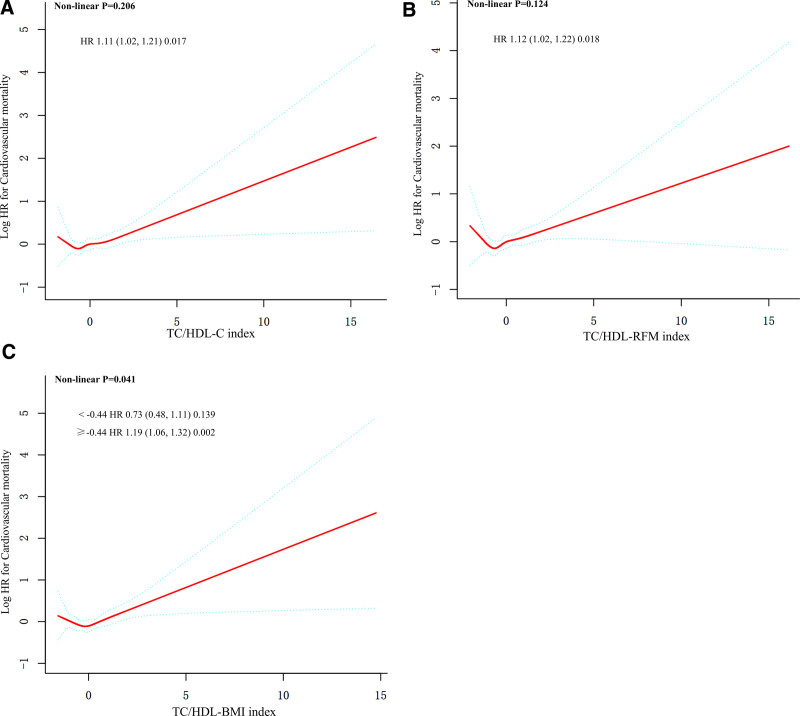
The relationship between the total cholesterol/high-density lipoprotein cholesterol (TC/HDL) and TC/HDL with the combination of obesity indicators and obstructive sleep apnea (OSA) remains unclear. Therefore, we aimed to explore the associations between TC/HDL-related indices and OSA as well as clinical outcomes. This study enrolled 20,076 patients from the National Health and Nutrition Examination Survey (2005-2008 and 2015-2018). Three indicators were constructed including TC/HDL index, TC/HDL combining with relative fat mass (TC/HDL-RFM), and TC/HDL combining with body mass index (TC/HDL-BMI). We performed multivariable logistic regression and generalized additive models to evaluate the association between TC/HDL-related indices and OSA. Multivariable Cox proportional hazards regression models with restricted cubic splines were performed to assess the relationships between TC/HDL-related indices and mortality. Stratified analyses were conducted to further investigate population-specific differences. The multivariable logistic regression analyses showed that high levels of TC/HDL-related indices were significantly associated with increased prevalences of OSA (TC/HDL: odds ratio [OR] per 1 standard deviation [SD] increase: 1.1, 95% confidence interval [CI]: 1.07-1.14, P < .001; TC/HDL-RFM: OR per 1SD increase: 1.22, 95% CI: 1.18-1.27, P < .001; TC/HDL-BMI: OR per 1SD increase: 1.28, 95% CI: 1.23-1.33, P < .001). Inverted U-shaped curves were depicted between TC/HDL-related indices and OSA. During a mean follow-up of 91 months, 1917 (9.5%) all-cause deaths occurred, and 567 (2.8%) were contributed to cardiovascular deaths. Meanwhile, the TC/HDL-related indices were associated with cardiovascular mortality, but not with all-cause mortality. Subgroup analyses showed that the strength of this relationship was found to be more pronounced in participants with OSA. The TC/HDL-related indices were independent predictors of OSA and cardiovascular mortality. Our study indicated that TC/HDL-related indices can assist clinicians in making more informed clinical decisions for patients with OSA and help reduce the risk of cardiovascular mortality.
Keywords: TC/HDL; TC/HDL-BMI; TC/HDL-RFM; cardiovascular mortality; obstructive sleep apnea.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures





References
-
- Seetho IW, Parker RJ, Craig S, Duffy N, Hardy KJ, Wilding JPH. Obstructive sleep apnea is associated with increased arterial stiffness in severe obesity. J Sleep Res. 2014;23:700–8. - PubMed
-
- Vavougios GD, George DG, Pastaka C, Zarogiannis SG, Gourgoulianis KI. Phenotypes of comorbidity in OSAS patients: combining categorical principal component analysis with cluster analysis. J Sleep Res. 2016;25:31–8. - PubMed
-
- Almendros I, Basoglu K, Conde SV, Liguori C, Saaresranta T. Metabolic dysfunction in OSA: is there something new under the sun? J Sleep Res. 2022;31:e13418. - PubMed
-
- Kastelein JJ, van der Steeg WA, Holme I, et al. ; TNT Study Group. Lipids, apolipoproteins, and their ratios in relation to cardiovascular events with statin treatment. Circulation. 2008;117:3002–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
