

Muscle weakness after critical illness: unravelling biological mechanisms and clinical hurdles
- PMID: 40528196
- PMCID: PMC12175454
- DOI: 10.1186/s13054-025-05462-z
Muscle weakness after critical illness: unravelling biological mechanisms and clinical hurdles
Abstract
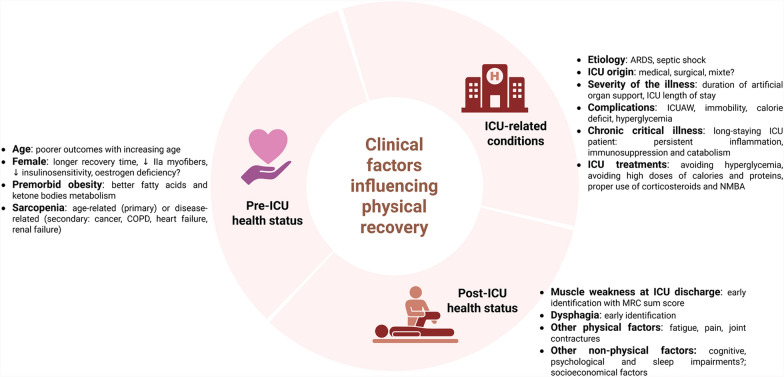
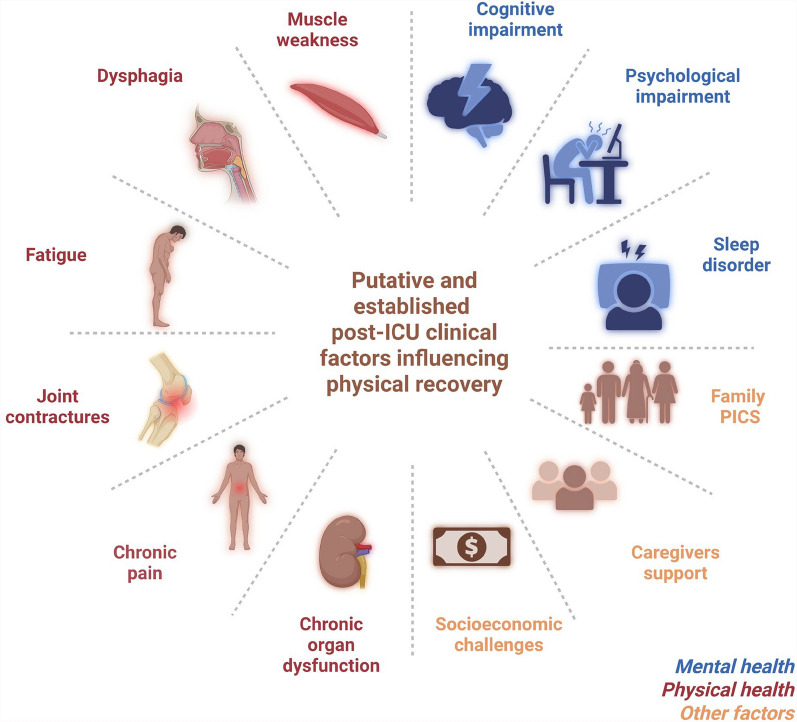
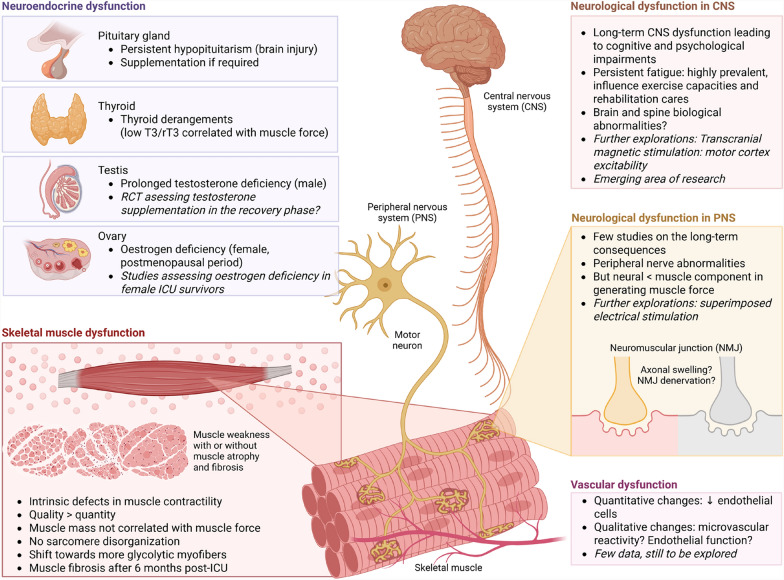
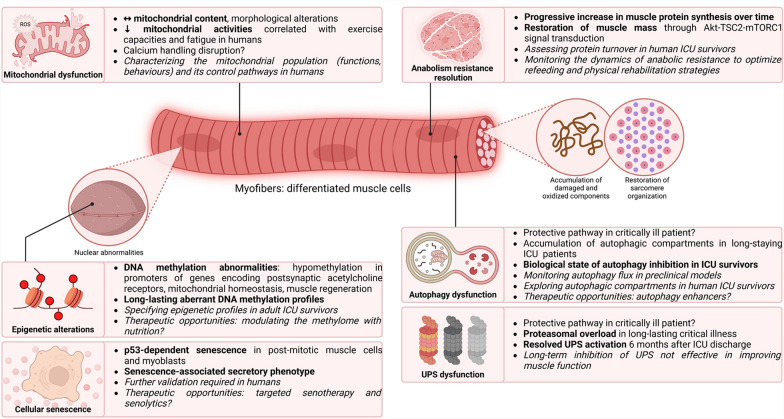
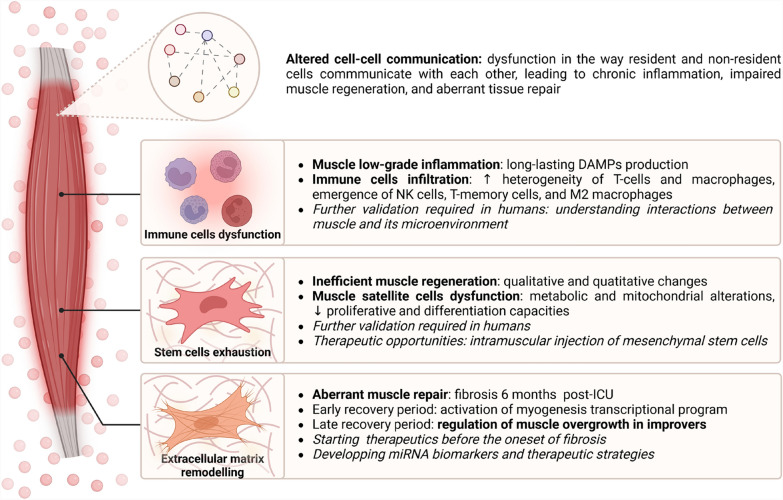
Survivors of intensive care unit (ICU) are increasingly numerous because of better hospital care. However, several consequences of an ICU stay, known as post-intensive care syndrome, worsen long-term prognoses. A predominant feature in survivors is reduced muscle strength, mass, and physical function. This leads to lower exercise capacity, long-lasting physical disability, higher mortality risk, and subsequent health costs. While ICU-acquired muscle weakness has been extensively studied these past decades, underlying mechanisms of post-ICU muscle weakness remain poorly understood, and there is still no evidence-based treatment for improving long-term physical outcomes. One hypothesis, among others, could be that the pathophysiology is dynamic over time, differing between the acute ICU and post-ICU recovery periods. This narrative review aims to address the clinical, physiological and biological determinants of persistent muscle dysfunction in ICU survivors, with particular attention to the molecular, cellular and systemic mechanisms involved. Specifically, pre-ICU health factors such as obesity and sarcopenia, ICU-related complications and treatments, and post-ICU management all influence recovery. Dysfunctions in the neuroendocrine, vascular, neurological, and muscle systems contribute as physiological determinants of the muscle weakness. Complex and multifaceted biological mechanisms drive the post-ICU muscle dysfunction with mitochondrial and autophagy dysfunction, epigenetic modifications, cellular senescence, muscle inflammation with altered cell-cell communication, including dysfunction of immune cells, stem cell exhaustion and extracellular matrix remodelling. The review also sheds light on new and innovative therapeutic approaches and discusses future research directions. Emphasis is placed on the potential for multi-approach treatments that integrate nutritional, physical, and biological interventions. Addressing these aspects in a holistic and dynamic manner, from ICU to post-ICU phases, may provide avenues for mitigating the long-term burden of muscle weakness and physical disability in ICU survivors.
Keywords: ICU survivors; Long-term outcome; Muscle weakness; Post-ICU syndrome; Translational research.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
