

Nonsuicidal self-injury prediction with pain-processing neural circuits using interpretable graph neural network
- PMID: 40528360
- PMCID: PMC12180354
- DOI: 10.1080/07853890.2025.2520394
Nonsuicidal self-injury prediction with pain-processing neural circuits using interpretable graph neural network
Abstract
Background: Nonsuicidal self-injury (NSSI) involves the intentional destruction of one's own body tissues without suicidal intent. Prior research has shown that individuals with NSSI exhibit abnormal pain perception; however, the pain-processing neural circuits underlying NSSI remain poorly understood. This study leverages graph neural networks to predict NSSI risk and examine the learned connectivity of neural underpinnings using multimodal data.
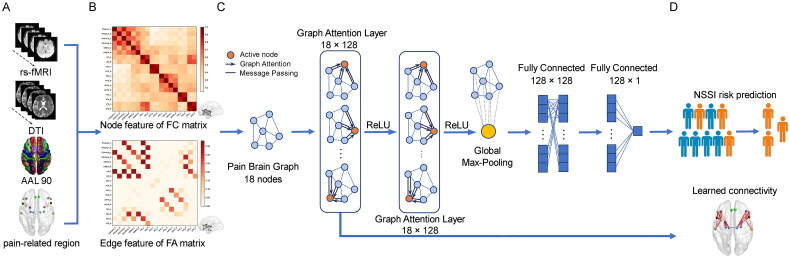
Methods: Resting-state functional MRI and diffusion tensor imaging were collected from 50 patients with NSSI, 79 healthy controls (HC), and 44 patients with mental disorder who did not engage in NSSI as disease controls (DC). We constructed pain-related brain networks for each participant. An interpretable graph attention networks (GAT) model was developed, considering demographic factors, to predict NSSI risk and highlight NSSI-specific connectivity using learned attention matrices.
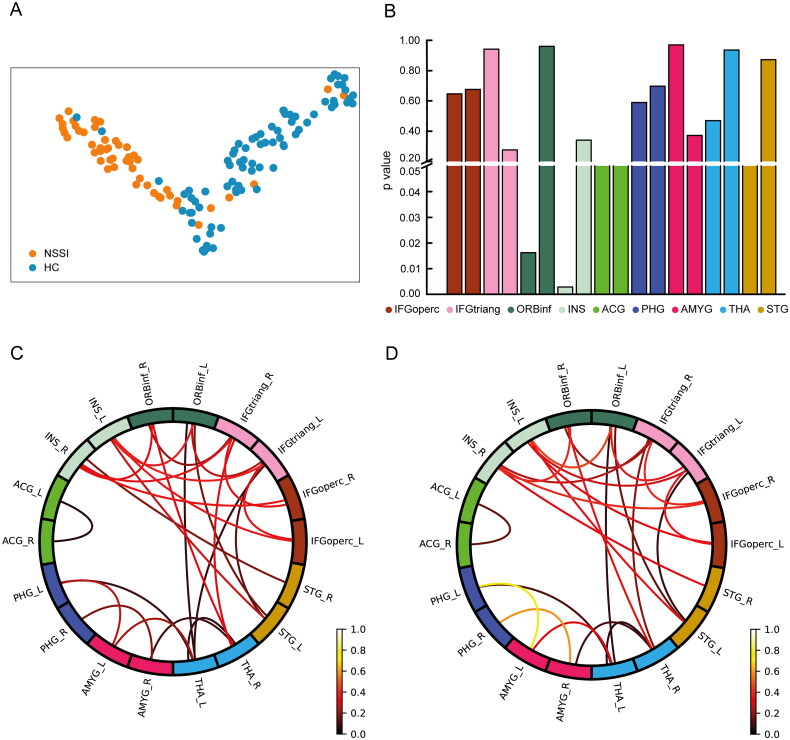
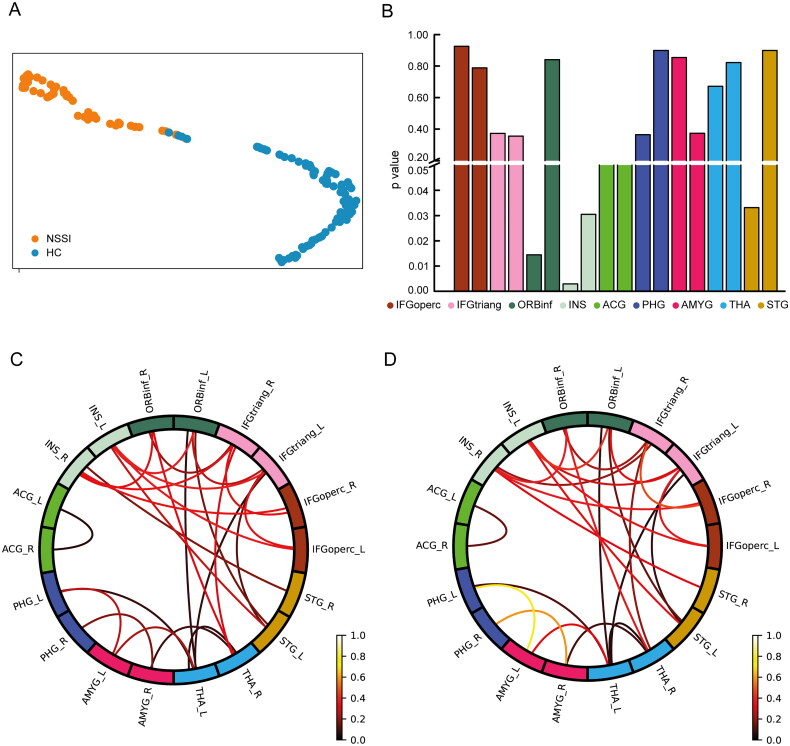
Results: The proposed GAT model based on imaging data achieved an accuracy of 80%, and increased to 88% when self-reported pain scales were incorporated alongside imaging data in distinguishing patients with NSSI from HC. It highlighted amygdala-parahippocampus and inferior frontal gyrus (IFG)-insula connectivity as pivotal in NSSI-related pain processing. After incorporating imaging data of DC, the model's accuracy reached 74%, underscoring consistent neural connectivity patterns. The GAT model demonstrates high predictive accuracy for NSSI, enhanced by including self-reported pain scales.
Conclusions: Our proposed GAT model underscores the significance in the functional integration of limbic regions, paralimbic regions and IFG in NSSI pain processing. Our findings suggest altered pain processing as a key mechanism in NSSI, providing insights for potential neural modulation intervention strategies.
Keywords: Nonsuicidal self-injury; functional magnetic resonance imaging; graph attention networks; graph neural networks; interpretable machine learning; pain-processing neural circuits.
Conflict of interest statement
No potential competing interest was reported by the authors.
Figures
References
-
- Zhang P, Ouyang L, Liang M, et al. A cross-sectional epidemiological study of non-suicidal self-injury prevalence in Chinese psychiatric patients. Nat Mental Health. 2023;1(4):266–272. doi: 10.1038/s44220-023-00050-y. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical