

Patient-generated health data: Impact on promoting patient-centered point of care tobacco treatment in patients with cancer
- PMID: 40529004
- PMCID: PMC12171923
- DOI: 10.1017/cts.2025.77
Patient-generated health data: Impact on promoting patient-centered point of care tobacco treatment in patients with cancer
Abstract
Introduction: Guideline-based tobacco treatment is infrequently offered. Electronic health record-enabled patient-generated health data (PGHD) has the potential to increase patient treatment engagement and satisfaction.
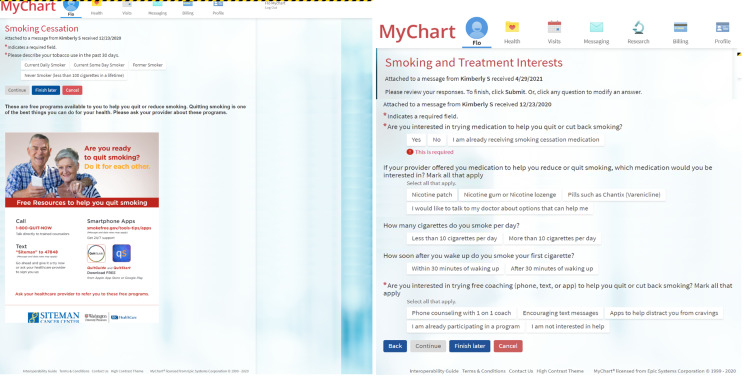
Methods: We evaluated outcomes of a strategy to enable PGHD in a medical oncology clinic from July 1, 2021 to December 31, 2022. Among 12,777 patients, 82.1% received a tobacco screener about use and interest in treatment as part of eCheck-in via the patient portal.
Results: We attained a broad reach (82.1%) and moderate response rate (30.9%) for this low-burden PGHD strategy. Patients reporting current smoking (n = 240) expressed interest in smoking cessation medication (47.9%) and counseling (35.8%). As a result of patient requests via PGHD, most tobacco treatment requests by patients were addressed by their providers (40.6-80.3%). Among patients with active smoking, those who received/answered the screener (n = 309 ) were more likely to receive tobacco treatment compared with usual care patients who did not have the patient portal (n = 323) (OR = 2.72, 95% CI = 1.93-3.82, P < 0.0001) using propensity scores to adjust for the effect of age, sex, race, insurance, and comorbidity. Patients who received yet ignored the screener (n = 1024) compared with usual care were also more likely to receive tobacco treatment, but to a lesser extent (OR = 2.20, 95% CI = 1.68-2.86, P < 0.0001). We mapped observed and potential benefits to the Translational Science Benefits Model (TSBM).
Discussion: PGHD via patient portal appears to be a feasible, acceptable, scalable, and cost-effective approach to promote patient-centered care and tobacco treatment in cancer patients. Importantly, the PGHD approach serves as a real world example of cancer prevention leveraging the TSBM.
Keywords: Patient-generated health data; cancer prevention; health informatics; tobacco treatment; translation.
© The Author(s) 2025.
Conflict of interest statement
Dr Bierut is listed as inventor on issued U.S. patent 8,080,371, “Markers for Addiction” covering the use of certain SNPs in determining the diagnosis, prognosis, and treatment of addiction. All other authors declare no potential conflict of interest. Dr Baker has a Glaxo-Wellcome Chair in the Department of Medicine.
Figures




References
-
- Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention (US); 2010. 5, Cancer. Available from: https://www.ncbi.nlm.nih.gov/books/NBK53010/. - PubMed
-
- Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion. Website accessed on 1/31/2024: https://www.cdc.gov/vitalsigns/cancerandtobacco/index.html.
-
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014 [accessed 2022 Feb 7].
LinkOut - more resources
Full Text Sources
Research Materials