

Mirizzi syndrome masquerading as gallbladder carcinoma: a case report on diagnostic challenges and multidisciplinary management
- PMID: 40529141
- PMCID: PMC12171177
- DOI: 10.3389/fmed.2025.1586112
Mirizzi syndrome masquerading as gallbladder carcinoma: a case report on diagnostic challenges and multidisciplinary management
Abstract
Background: Mirizzi syndrome is a rare condition that is frequently misdiagnosed as gallbladder cancer due to overlapping clinical and imaging features. This case underscores the diagnostic challenge of differentiating these two conditions and offers insights into managing such complex presentations.
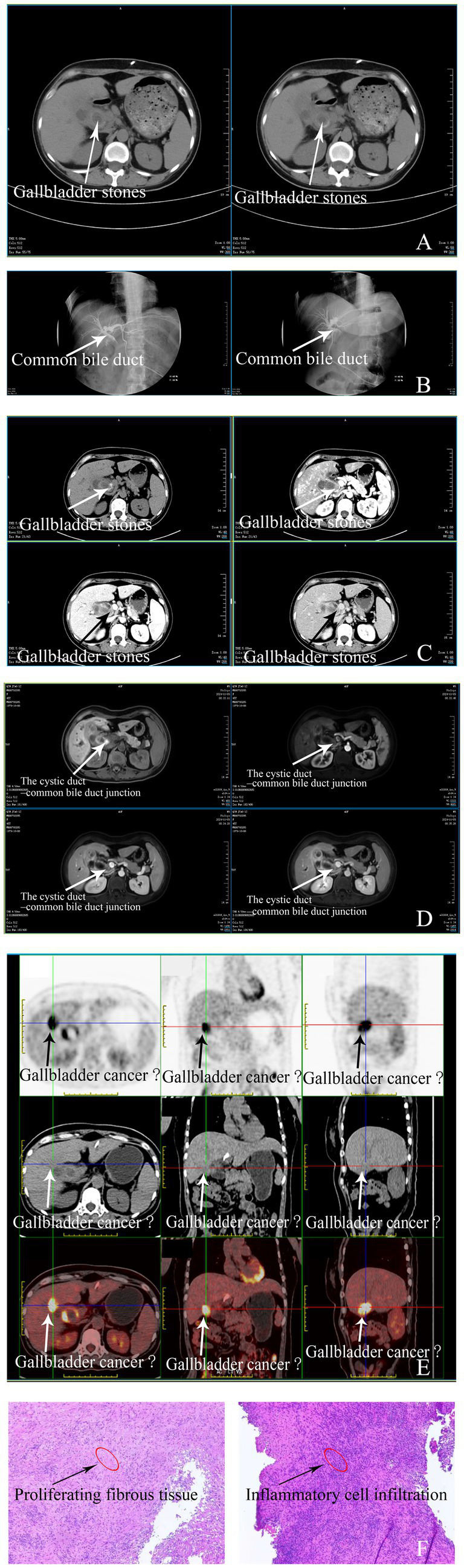
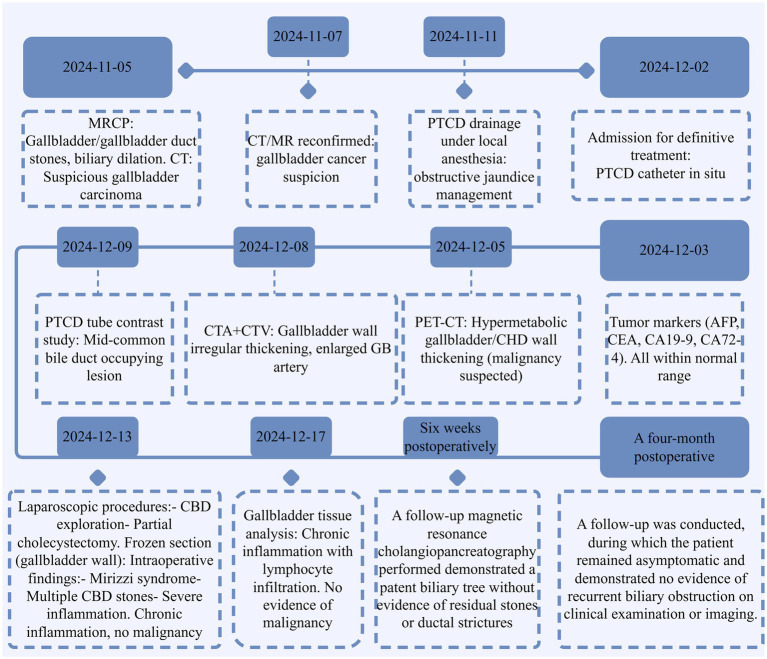
Case summary: A 45-year-old female presented with obstructive jaundice and elevated liver enzymes. Imaging studies, including CT, PET-CT, and MRCP, revealed gallbladder wall thickening, bile duct obstruction, and a high suspicion of malignancy. Tumor markers were within normal limits. Intraoperatively, extensive adhesions, gallbladder wall oedema, and bile duct compression consistent with Mirizzi syndrome were identified. A partial cholecystectomy and bile duct exploration with stent placement were performed. Histopathological examination confirmed chronic cholecystitis with inflammation, but no evidence of malignancy. The patient had an uneventful recovery, with complete resolution of her symptoms.
Conclusion: Mirizzi syndrome can closely resemble gallbladder cancer, making careful surgical exploration and pathological evaluation essential for accurate diagnosis.
Keywords: Mirizzi syndrome; case report; cholangitis; gallbladder cancer; obstructive jaundice.
Copyright © 2025 Yang, Hou, Yi, Zhou, Tang, Fu, Hu and Xing.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Mirizzi Syndrome: The Uncommon and Overlooked Surgical Cause of Obstructive Jaundice.Cureus. 2025 Jun 9;17(6):e85611. doi: 10.7759/cureus.85611. eCollection 2025 Jun. Cureus. 2025. PMID: 40636631 Free PMC article.
-
A Case of Jaundice Revealing a Hidden Duo: Lemmel's Syndrome and a Duplicated Gallbladder.Cureus. 2025 Jun 11;17(6):e85766. doi: 10.7759/cureus.85766. eCollection 2025 Jun. Cureus. 2025. PMID: 40656420 Free PMC article.
-
Imaging Findings of Mirizzi Syndrome Associated With Acalculous Cholecystitis: A Case Report.Cureus. 2025 Jan 30;17(1):e78261. doi: 10.7759/cureus.78261. eCollection 2025 Jan. Cureus. 2025. PMID: 40026964 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
Acute gallbladder pathologies beyond uncomplicated cholecystitis.Emerg Radiol. 2025 Aug;32(4):605-621. doi: 10.1007/s10140-025-02355-0. Epub 2025 Jun 10. Emerg Radiol. 2025. PMID: 40493308 Review.
References
-
- Hassan R, Solinas L, Notarangelo M, Sagnotta A, Giubilo C, Battaglia B, et al. Mirizzi syndrome: a challenging diagnosis. Case report. G Chir. (2019) 40:193–8. - PubMed
-
- Jones MW, Ferguson T. Mirizzi Syndrome. Treasure Island (FL): StatPearls Publishing; (2024). - PubMed
-
- Cai Y, Fan Z, Yang G, Zhao D, Shan L, Lin S, et al. Analysis of the efficacy of percutaneous Transhepatic cholangiography drainage (PTCD) and endoscopic retrograde cholangiopancreatography (ERCP) in the treatment of malignant obstructive jaundice (MOJ) in palliative drainage and preoperative biliary drainage: a single-center retrospective study. BMC Surg. (2024) 24:307. doi: 10.1186/s12893-024-02595-w, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources