

A gene expression-based approach for the precision use of hydrocortisone in septic shock patients; a secondary analysis of the ADRENAL trial
- PMID: 40529301
- PMCID: PMC12173105
- DOI: 10.1016/j.ccrj.2025.100109
A gene expression-based approach for the precision use of hydrocortisone in septic shock patients; a secondary analysis of the ADRENAL trial
Abstract
Background: Small observational studies suggest the effect of corticosteroids in patients with vasodilatory shock vary depending on endotypes determined by gene expression. We sought to replicate these findings in a larger cohort from a randomised clinical trial.
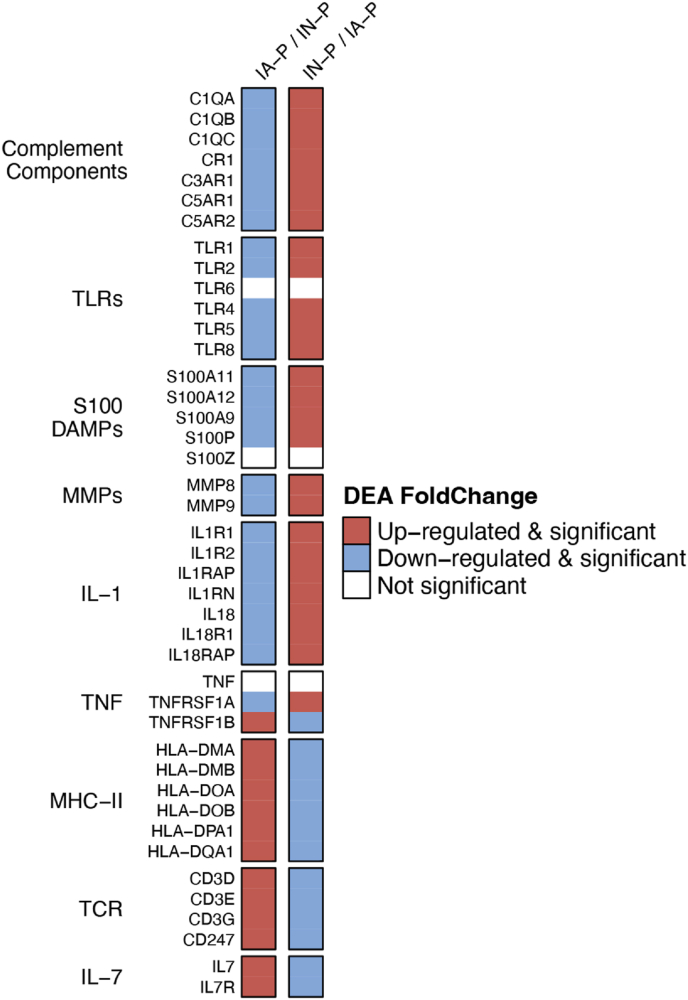
Methods: In a cross-sectional substudy of the Adjunctive Glucocorticoid Therapy In Septic Shock (ADRENAL) trial, patients were classified as one of two immune endotypes using predefined gene expression signatures: immune adaptive-prevalent (IA-P) or immune innate-prevalent (IN-P). We compared the outcomes of the two endotypes using a Bayesian analysis. The primary outcome was Day-28 mortality.
Findings: Of 540 patients, 267 (49.4%) were classified as IA-P and 273 (50.6%) as IN-P. In a Bayesian analysis using noninformative priors, there was no difference in the effect of hydrocortisone on 28-day mortality (odds ratio [OR] 1.43, 95% credible intervals [CrI] 0.72-2.87) and OR 1.39, 95% CrI 0.74-2.61, between the IA-P and IN-P groups, respectively. In the subgroup of patients with more severe shock (n = 215/540, 40%), the corresponding figures for IA-P and IN-P were 1.21, 95% CrI (0.31-4.74) and OR 0.72 (95% CrI 0.30-1.67), respectively. In the subgroup of patients with pulmonary sepsis (232/540, 43%), IA-P patients treated with hydrocortisone had increased mortality (OR 5.55, 95% CrI 1.81-21.2).
Interpretation: Gene expression data from patients with septic shock reveal distinct immune endotypes. There was no evidence of a heterogeneity of treatment effect of hydrocortisone on mortality in the 2 endotypes or in the subgroup with severe shock. Patients with the IA-P endotype and pulmonary sepsis appear to be harmed by corticosteroids.
Keywords: Corticosteroids; Endotypes; RNA-Seq; Septic shock; Transcriptomics.
© 2025 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Balasubramanian Venkatesh reports financial support was provided by The George Institute for Global Health. Balasubramanian Venkatesh reports a relationship with The George Institute for Global Health that includes: funding grants. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Molecular feature-based classification of retroperitoneal liposarcoma: a prospective cohort study.Elife. 2025 May 23;14:RP100887. doi: 10.7554/eLife.100887. Elife. 2025. PMID: 40407808 Free PMC article.
-
Prenatal administration of progestogens for preventing spontaneous preterm birth in women with a multiple pregnancy.Cochrane Database Syst Rev. 2019 Nov 20;2019(11):CD012024. doi: 10.1002/14651858.CD012024.pub3. Cochrane Database Syst Rev. 2019. PMID: 31745984 Free PMC article.
-
Use of β-adrenoreceptor drugs and Parkinson's disease incidence in women from the French E3N cohort study.J Parkinsons Dis. 2025 Jun;15(4):789-804. doi: 10.1177/1877718X251330993. Epub 2025 Apr 29. J Parkinsons Dis. 2025. PMID: 40302366
-
Incidence of checkpoint inhibitor-associated inflammatory arthritis, immunomodulation and mortality in cancer patients on immunotherapy: a retrospective cohort study.Rheumatology (Oxford). 2025 Apr 1;64(4):1637-1642. doi: 10.1093/rheumatology/keae343. Rheumatology (Oxford). 2025. PMID: 38889288 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
References
-
- Reinhart K., Daniels R., Kissoon N., Machado F.R., Schachter R.D., Finfer S. Recognizing sepsis as a Global Health Priority - A WHO Resolution. N Engl J Med. 2017;377(5):414–417. - PubMed
-
- Venkatesh B., Finfer S., Cohen J., Rajbhandari D., Arabi Y., Bellomo R., et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378(9):797–808. - PubMed
-
- Annane D., Renault A., Brun-Buisson C., Megarbane B., Quenot J.P., Siami S., et al. Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378(9):809–818. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
