

Predicting Stroke-Associated Pneumonia in Acute Ischemic Stroke: A Machine Learning Model Development and Validation Study with CBC-Derived Inflammatory Indices
- PMID: 40529346
- PMCID: PMC12170845
- DOI: 10.2147/IJGM.S524450
Predicting Stroke-Associated Pneumonia in Acute Ischemic Stroke: A Machine Learning Model Development and Validation Study with CBC-Derived Inflammatory Indices
Abstract
Purpose: Stroke-associated pneumonia (SAP), a critical complication of ischemic stroke, significantly worsens outcomes. Our aim was to identify SAP risk factors and develop a machine learning (ML) model for early risk stratification.
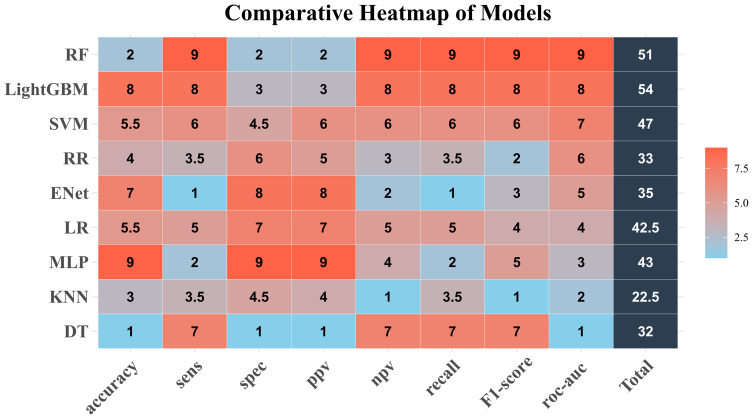
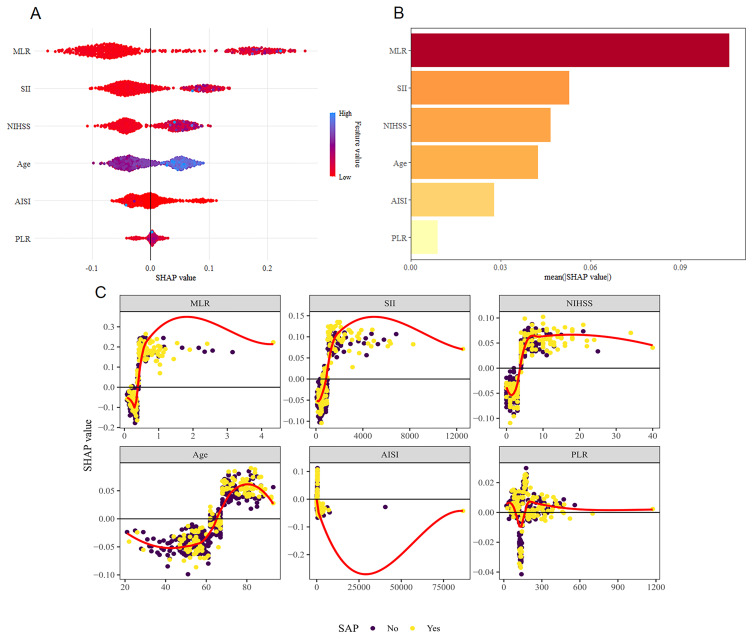
Methods: This retrospective study analyzed 574 ischemic stroke patients, divided into training (75%) and testing (25%) sets. Nine ML models were trained using 10-fold cross-validation, with performance evaluated by accuracy, AUC-ROC, and F1-score. Key predictors were interpreted via SHAP analysis. An interactive web tool was developed using the optimal model.
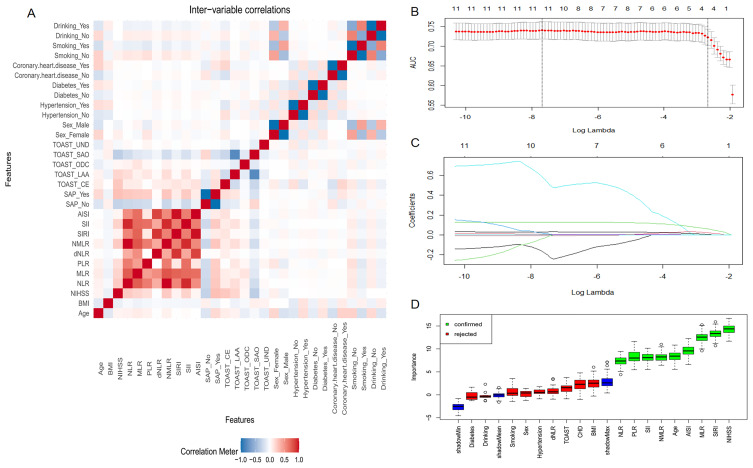
Results: SAP incidence was 32.4%. LightGBM demonstrated superior predictive performance (ranking score=54) without overfitting, identifying Monocyte-to-lymphocyte ratio (MLR), systemic immune-inflammation index (SII), NIHSS score, age, aggregate index of systemic inflammation (AISI), and platelet-to-lymphocyte ratio (PLR) as the top predictors.
Conclusion: Our findings demonstrate that machine learning models exhibit strong predictive performance for SAP, with the LightGBM algorithm outperforming other approaches. The web-based prediction tool developed from this model provides clinicians with actionable insights to support real-time clinical decision-making.
Keywords: ischemic stroke; machine learning; stroke-associated pneumonia.
© 2025 Xie et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Wang YJ, Li ZX, Gu HQ, et al. China stroke statistics: an update on the 2019 report from the national center for healthcare quality management in neurological diseases, China national clinical research center for neurological diseases, the Chinese stroke association, national center for chronic and non-communicable disease control and prevention, Chinese center for disease control and prevention and institute for global neuroscience and stroke collaborations. Stroke Vasc Neurol. 2022;7(5):415–450. doi: 10.1136/svn-2021-001374 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
