

Autoimmune Diseases: Molecular Pathogenesis and Therapeutic Targets
- PMID: 40529617
- PMCID: PMC12171081
- DOI: 10.1002/mco2.70262
Autoimmune Diseases: Molecular Pathogenesis and Therapeutic Targets
Abstract
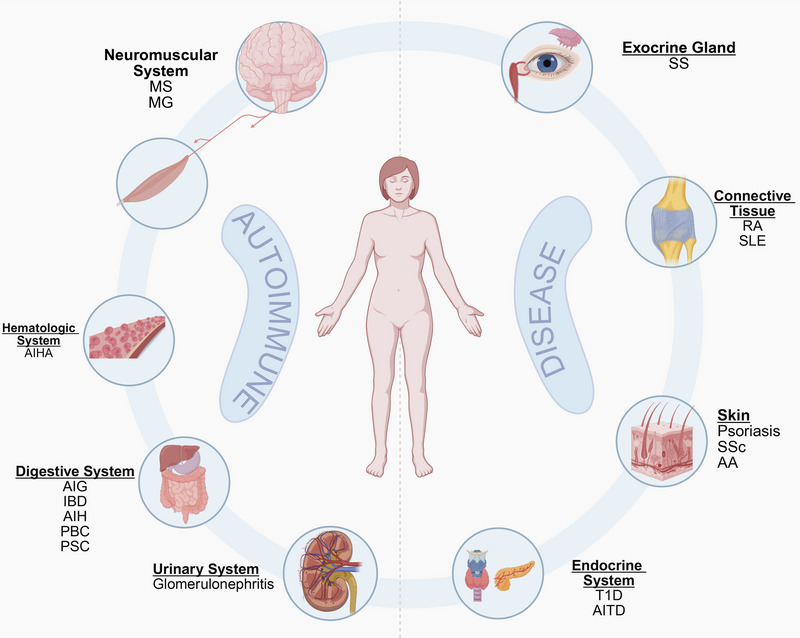
Autoimmune diseases are a set of disorders in which the immune system attacks one's own tissues, leading to chronic inflammation, tissue damage, and systemic dysfunction. Affecting approximately 10% of the global population, these diseases impose significant health and economic burdens worldwide. The pathogenesis of autoimmune diseases is complex, involving not only genetic predisposition (e.g., human leukocyte antigen variants), environmental triggers (e.g., infections), and a dysregulated immune response but also various interacting components that contribute to the development of diverse clinical phenotypes. This review provides a comprehensive overview of common autoimmune diseases, covering their clinical manifestations, pathogenic mechanisms, and diagnostic approaches such as disease-specific autoantibodies. We also explore current therapeutic strategies, including commonly used broad-spectrum anti-inflammatory drugs, recent molecular-targeted therapies (e.g., Janus kinase inhibitors, monoclonal antibodies), and emerging cellular therapies such as chimeric antigen receptor T cells therapy and regulatory T-cell adoptive transfer. Incorporating knowledge from preclinical and clinical studies, this review synthesizes relevant information to inform about autoimmune diseases, bridge the gap from lab to clinic, and promote future advances through exploring precision medicine applications to meet clinical needs.
Keywords: autoimmune diseases; immune tolerance; pathogenesis; therapeutic strategies.
© 2025 The Author(s). MedComm published by Sichuan International Medical Exchange & Promotion Association (SCIMEA) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
Surveillance for Violent Deaths - National Violent Death Reporting System, 50 States, the District of Columbia, and Puerto Rico, 2022.MMWR Surveill Summ. 2025 Jun 12;74(5):1-42. doi: 10.15585/mmwr.ss7405a1. MMWR Surveill Summ. 2025. PMID: 40493548 Free PMC article.
-
Understanding and Overcoming Negative Attitudes That Hinder Adoption of Reablement in Dementia Care: An Explorative Qualitative Study.J Multidiscip Healthc. 2025 Jun 12;18:3411-3422. doi: 10.2147/JMDH.S522515. eCollection 2025. J Multidiscip Healthc. 2025. PMID: 40534647 Free PMC article.
-
Disease association study of Autoimmune and autoinflammatory diseases by integrating multi-modal data and hierarchical ontologies.Front Immunol. 2025 Jun 4;16:1575490. doi: 10.3389/fimmu.2025.1575490. eCollection 2025. Front Immunol. 2025. PMID: 40534874 Free PMC article.
-
Radiation-induced injury and the gut microbiota: insights from a microbial perspective.Therap Adv Gastroenterol. 2025 Jun 16;18:17562848251347347. doi: 10.1177/17562848251347347. eCollection 2025. Therap Adv Gastroenterol. 2025. PMID: 40535532 Free PMC article. Review.
References
-
- Wang L., Wang F., and Gershwin M. E., “Human Autoimmune Diseases: A Comprehensive Update,” Journal of Internal Medicine 278, no. 4 (2015): 369–395. - PubMed
-
- Conrad N., Misra S., Verbakel J. Y., et al., “Incidence, Prevalence, and co‐occurrence of Autoimmune Disorders Over Time and by Age, Sex, and Socioeconomic Status: A Population‐based Cohort Study of 22 Million Individuals in the UK,” The Lancet 401, no. 10391 (2023): 1878–1890. - PubMed
-
- Cao F., He Y., Wang Y., et al., “Global Burden and Cross‐country Inequalities in Autoimmune Diseases From 1990 to 2019,” Autoimmunity Reviews 22, no. 6 (2023): 103326. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous