

The implementation effect of DIP payment method across different population in Southwest China based on multi-group interrupt time series
- PMID: 40529706
- PMCID: PMC12171191
- DOI: 10.3389/fpubh.2025.1572475
The implementation effect of DIP payment method across different population in Southwest China based on multi-group interrupt time series
Abstract
Background: Since 2020, China has implemented a payment method known as "Diagnosis-Intervention Package" (DIP) in 71 cities nationwide to address the specific needs of the country. The objective of this study is to evaluate the impact of DIP on medical quality and the burden experienced by inpatients covered under the Urban Employee Basic Medical Insurance (UEBMI) and Urban and Rural Residents Basic Medical Insurance (URRBMI). Furthermore, it aims to investigate potential differences in these effects between inpatients enrolled in the two distinct types of insurance, thereby enhancing our understanding of how this reform in payment methods influences healthcare delivery, and refine the social security system.
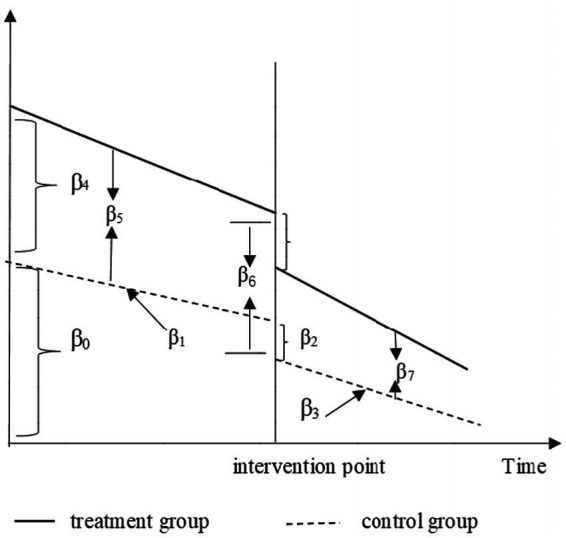
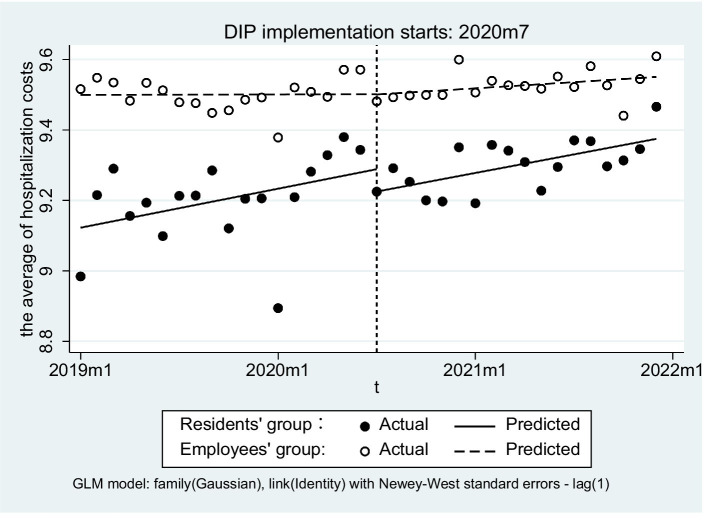
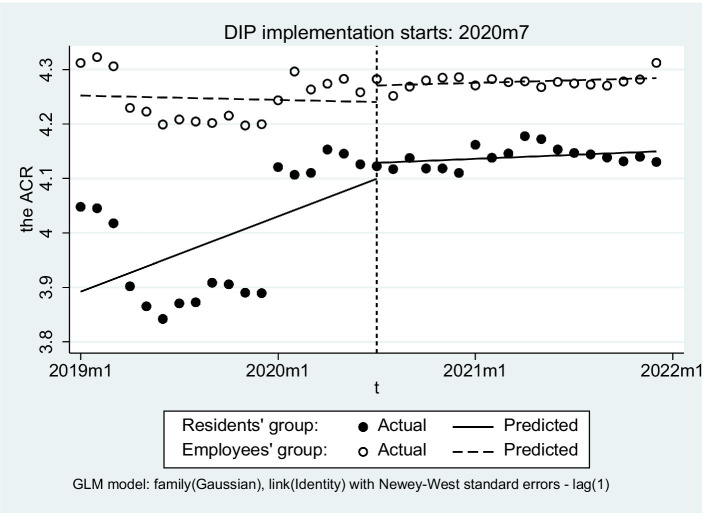
Methods: We conducted a multiple-group interrupted time series analyses (MGITSA) on outcome variables reflecting medical services quality, and the burden of UEBMI and URRBMI inpatients, based on a dataset containing 180,071 inpatient reimbursement records in City C spanning from January, 2019 to December, 2021. This dataset included 42,581 records for URRBMI inpatients and 137,490 records for UEBMI inpatients.
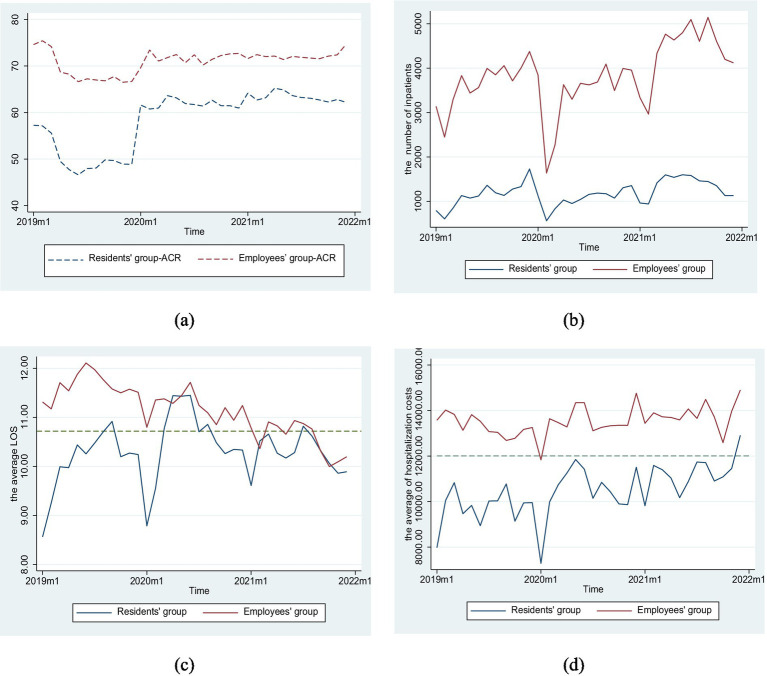
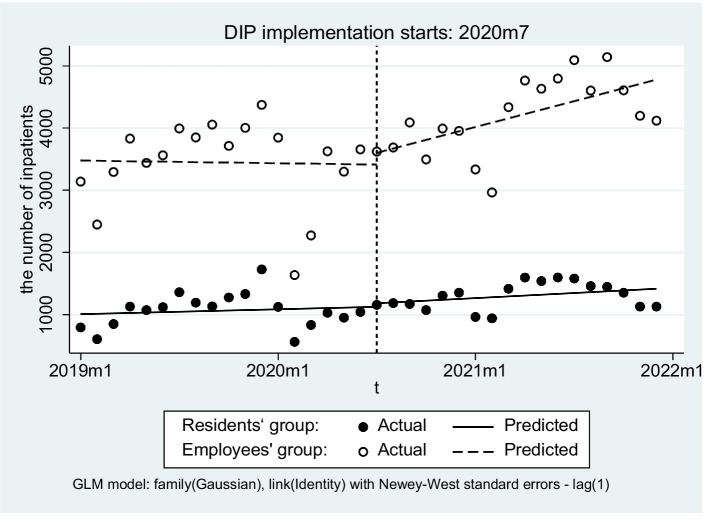
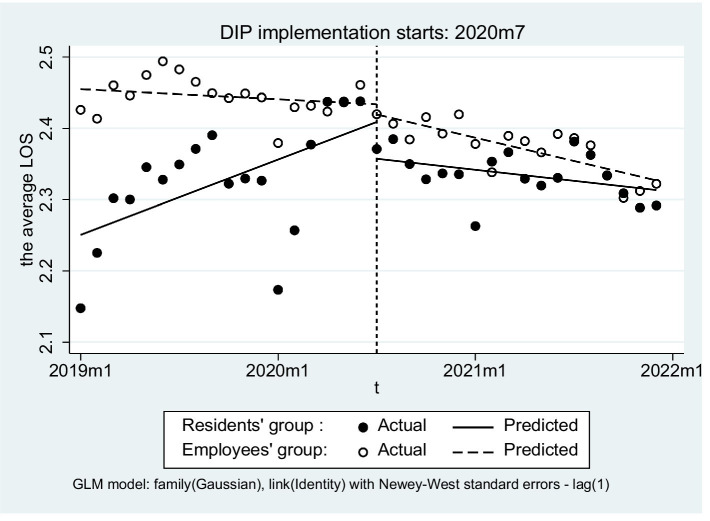
Results: After DIP implementation, both UEBMI and URRBMI showed increased inpatient numbers (21.59% and 22.26%, respectively), reduced LOS (7.10% for UEBMI, 0.29% for URRBMI), and higher ACR (3.07% for UEBMI, 15.36% for URRBMI). Hospitalization costs increased slightly for both groups (2.97% for UEBMI, 10.44% for URRBMI). Subgroup analysis revealed age-specific differences: significant LOS and cost changes in <18-year-olds and >45-year-olds, but minimal effects in 18-45-year-olds. MGITSA showed URRBMI experienced significant LOS reduction (β3=-0.004, P=0.014), while UEBMI had more pronounced LOS and ACR trends, with no significant inter-group differences in cost slopes.
Conclusion: DIP improved hospital efficiency (reduced LOS, increased admissions) and financial protection (higher ACR) for both insurance groups in the short term, though hospitalization costs rose, requiring attention to potential service intensity inflation or cost-shifting. Age disparities in DIP impacts highlight the need for targeted policies. Continuous monitoring and policy adjustments are essential to balance cost control, service quality, and equity, ensuring DIP's long-term effectiveness in China's healthcare reform.
Keywords: Diagnosis-Intervention Packet; mandatory medical insurance; medical efficiency; medical services quality; the burden of patients.
Copyright © 2025 Wu, Wu, Cao and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . (2024). Global spending on health coping with the pandemic [EB/OL]. Available online at: https://apps.who.int/nha/database (Accessed August 6, 2024).
-
- World Health Organization . The world health report: Health systems financing: the path to universal coverage. Geneva: World Health Organization; (2010). Available online at: https://iris.who.int/handle/10665/44371 (Accessed August 6, 2024). - PMC - PubMed
-
- National Healthcare Security Administration . (2024). Notice of the Office of the National Healthcare Security Administration on printing and distributing the 2.0 grouping plan for payment by disease group and disease type and deepening the relevant work [EB/OL]. Available online at: https://www.nhsa.gov.cn/art/2024/7/23/art_104_13313.html (Accessed August 16, 2024).
MeSH terms
LinkOut - more resources
Full Text Sources