

Splenic hypertrophy predicts liver-specific complications in patients undergoing major liver resection for colorectal liver metastases, after preoperative chemotherapy
- PMID: 40529910
- PMCID: PMC12170277
- DOI: 10.21037/hbsn-24-121
Splenic hypertrophy predicts liver-specific complications in patients undergoing major liver resection for colorectal liver metastases, after preoperative chemotherapy
Abstract
Background: In patients with colorectal liver metastases (CRLM), preoperative chemotherapy may increase resectability and survival outcomes. However, cytotoxic agents can also cause chemotherapy-associated liver injury (CALI), leading to increased rates of postoperative complications. This study evaluates the association between splenic hypertrophy (SH) after preoperative chemotherapy and postoperative liver-specific complications (LSC), in patients undergoing major liver resection for CRLM.
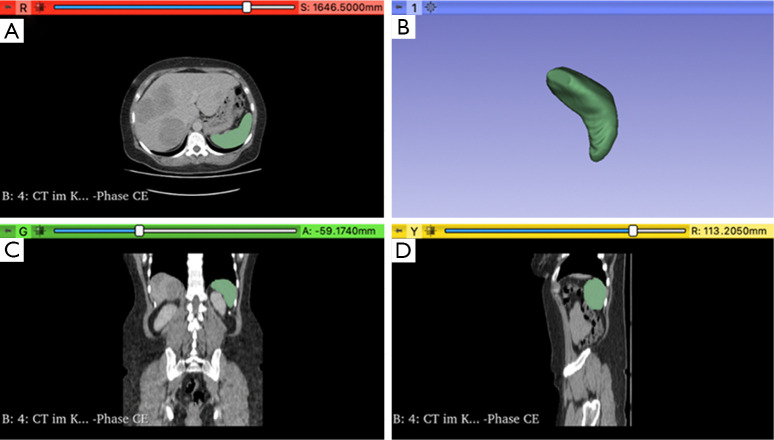
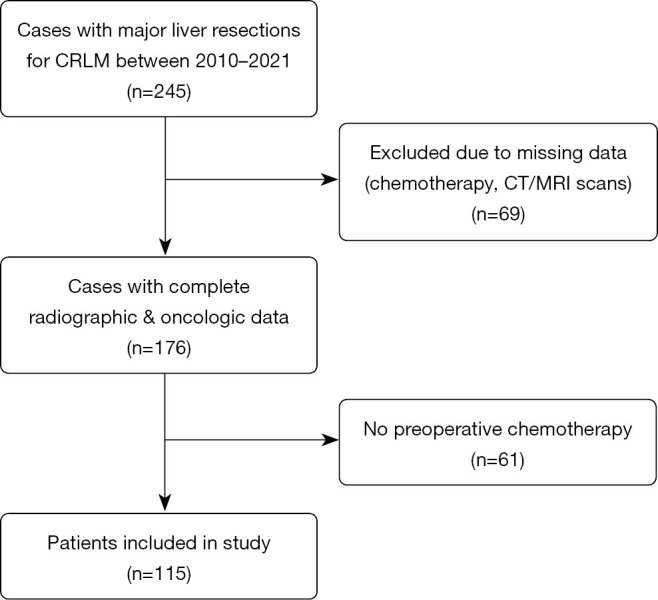
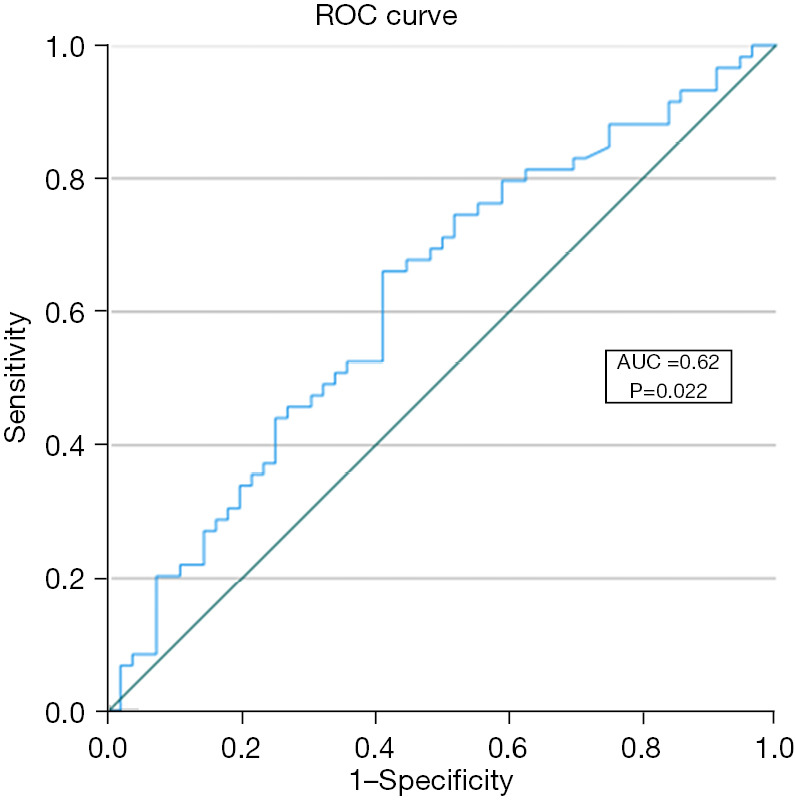
Methods: This retrospective study included patients who underwent major curative liver resection of CRLM following preoperative chemotherapy at the University Hospital RWTH Aachen (UH-RWTH) between 2010-2021. Patients with missing radiological images, incomplete data on chemotherapy regimens, or prior splenectomy were excluded. Volumetric measurements of the spleen were performed on preoperative computerized tomography (CT) and magnetic resonance imaging (MRI) images, using segmentation software (3D-Slicer). Receiver-operating characteristic (ROC) analysis was performed to determine the optimal SH cut-off for predicting postoperative LSC. Independent risk factors of postoperative LSC were examined using logistic regression.
Results: A total of 115 patients were included in the study, of which 78 (68%) received oxaliplatin as part of their preoperative chemotherapy regimen. A threshold of 8.6% SH (Youden Index =0.25) was identified as predictive of postoperative LSC. Patients with SH >8.6% (n=62) received oxaliplatin significantly more often (84% vs. 49%; P<0.001) and exhibited higher rates of liver fibrosis (72% vs. 52%, P=0.03) and LSC (63% vs. 38%, P=0.007). Multivariable logistic regression analysis identified SH >8.6% as an independent risk factor for LSC (odds ratio 2.86, 95% confidence interval: 1.104-7.402, P=0.03).
Conclusions: Preoperative SH may be a valuable predictor of postoperative LSC in patients undergoing major liver resection for CRLM, following chemotherapy. Further studies are necessary to investigate the impact on a larger cohort and find preventive strategies to mitigate and treat CALI.
Keywords: Colorectal liver metastases (CRLM); chemotherapy; splenic hypertrophy (SH); surgery.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-24-121/coif). D.T. reports honoraria from Bayer AG for lectures. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Systematic review of the influence of chemotherapy-associated liver injury on outcome after partial hepatectomy for colorectal liver metastases.Br J Surg. 2017 Jul;104(8):990-1002. doi: 10.1002/bjs.10572. Epub 2017 May 25. Br J Surg. 2017. PMID: 28542731
-
High Risk of Venous Thromboembolism With Aspirin Prophylaxis After THA for High-riding Developmental Dysplasia of the Hip: A Retrospective, Comparative Study.Clin Orthop Relat Res. 2025 Jun 9. doi: 10.1097/CORR.0000000000003482. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40536765
-
Return to Running After Achilles Tendon Repair: How Do US Navy Service Members' Physical Readiness Tests Change After Undergoing an Achilles Tendon Repair?Clin Orthop Relat Res. 2025 Jun 18. doi: 10.1097/CORR.0000000000003590. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40536551
-
Risk Factors for Postoperative Complications Following Resection of Colorectal Liver Metastases and the Impact on Long-Term Survival: A Population-Based National Cohort Study.World J Surg. 2023 Sep;47(9):2230-2240. doi: 10.1007/s00268-023-07043-z. Epub 2023 May 20. World J Surg. 2023. PMID: 37210422 Free PMC article.
-
Prevalence and odds of anxiety and depression in cutaneous malignant melanoma: a proportional meta-analysis and regression.Br J Dermatol. 2024 Jun 20;191(1):24-35. doi: 10.1093/bjd/ljae011. Br J Dermatol. 2024. PMID: 38197404
References
-
- Osterlund P, Salminen T, Soveri LM, et al. Repeated centralized multidisciplinary team assessment of resectability, clinical behavior, and outcomes in 1086 Finnish metastatic colorectal cancer patients (RAXO): A nationwide prospective intervention study. Lancet Reg Health Eur 2021;3:100049. 10.1016/j.lanepe.2021.100049 - DOI - PMC - PubMed
-
- Lam VW, Spiro C, Laurence JM, et al. A systematic review of clinical response and survival outcomes of downsizing systemic chemotherapy and rescue liver surgery in patients with initially unresectable colorectal liver metastases. Ann Surg Oncol 2012;19:1292-301. 10.1245/s10434-011-2061-0 - DOI - PubMed
LinkOut - more resources
Full Text Sources