

The Effects of Qigong and Tai Chi Exercises on Chronic Low Back Pain in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 40530198
- PMCID: PMC12173434
- DOI: 10.7759/cureus.84342
The Effects of Qigong and Tai Chi Exercises on Chronic Low Back Pain in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
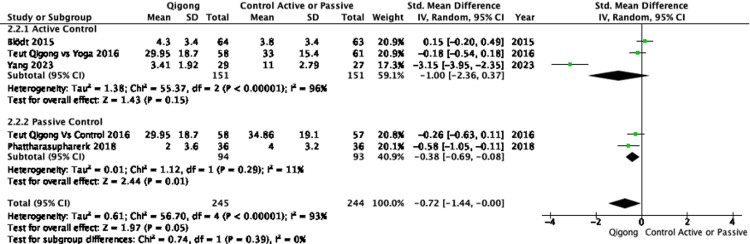
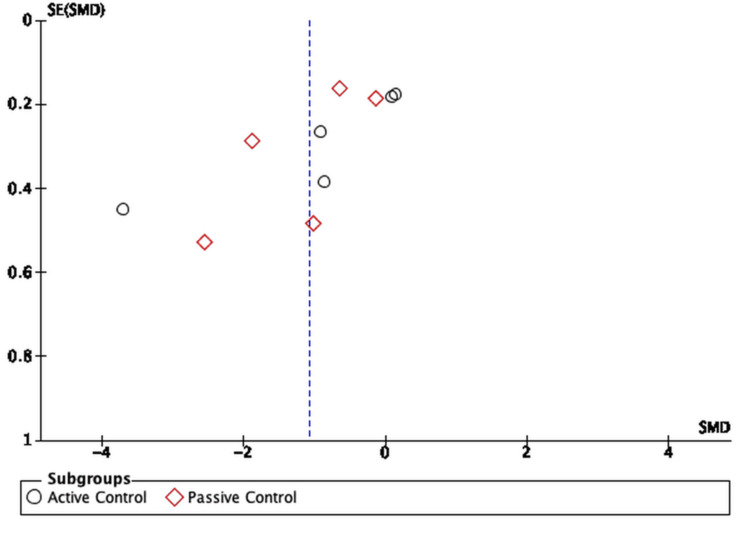
Qigong and Tai Chi are mind-body exercises that may provide therapeutic benefits for individuals with chronic low back pain (CLBP), yet their efficacy remains uncertain. This systematic review and meta-analysis assessed their effects on pain and disability in individuals with CLBP. Randomized controlled trials (RCTs) evaluating Qigong or Tai Chi for CLBP were included. A systematic search was conducted in MEDLINE (Medical Literature Analysis and Retrieval System Online), Embase, Physiotherapy Evidence Database (PEDro), and the Cochrane Library up to September 2023. Pain and disability were the primary outcomes. Risk of bias (RoB) was assessed independently by two reviewers using Cochrane's RoB 2 tool. The GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach was used to assess the certainty of the evidence. Eight RCTs (n = 729 adults, age range 31.5-73 years, intervention duration 4-24 weeks) were included. Meta-analysis was performed using a random-effects model, with heterogeneity quantified via I² statistics. Eight RCTs (n = 729 participants) were included. Qigong and Tai Chi significantly reduced pain intensity (standardized mean difference (SMD) = -1.07, 95%CI: -1.64 to -0.49, I² = 93%) and disability (SMD = -0.77, 95%CI: -1.39 to -0.15, I² = 93%) compared to control groups. Subgroup analyses suggested greater effect sizes against passive controls (SMD = -1.17, 95%CI: -1.91 to -0.43, I² = 90%) than against active controls (SMD = -0.98, 95%CI: -1.95 to -0.01, I² = 95%). Limitations include substantial heterogeneity among studies and imprecision in effect estimates. The certainty of evidence was rated moderate to high. Qigong and Tai Chi appear effective in reducing pain and disability in individuals with CLBP. However, substantial heterogeneity and the lack of direct comparisons with structured exercise programs necessitate further high-quality RCTs to confirm their long-term effectiveness.
Keywords: chronic low back pain (clbp); pain management; physiotherapy; qigong; systematic review and meta-analysis; taichi.
Copyright © 2025, Sotiropoulos et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures















References
-
- A systematic review of the global prevalence of low back pain. Hoy D, Bain C, Williams G, et al. Arthritis Rheum. 2012;64:2028–2037. - PubMed
-
- The burden of chronic low back pain: clinical comorbidities, treatment patterns, and health care costs in usual care settings. Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D. Spine (Phila Pa 1976) 2012;37:0–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources