

Gastric Volvulus as a Complication of Giant Hiatal Hernia: A Case Report and Literature Review
- PMID: 40530207
- PMCID: PMC12170235
- DOI: 10.7759/cureus.84257
Gastric Volvulus as a Complication of Giant Hiatal Hernia: A Case Report and Literature Review
Abstract
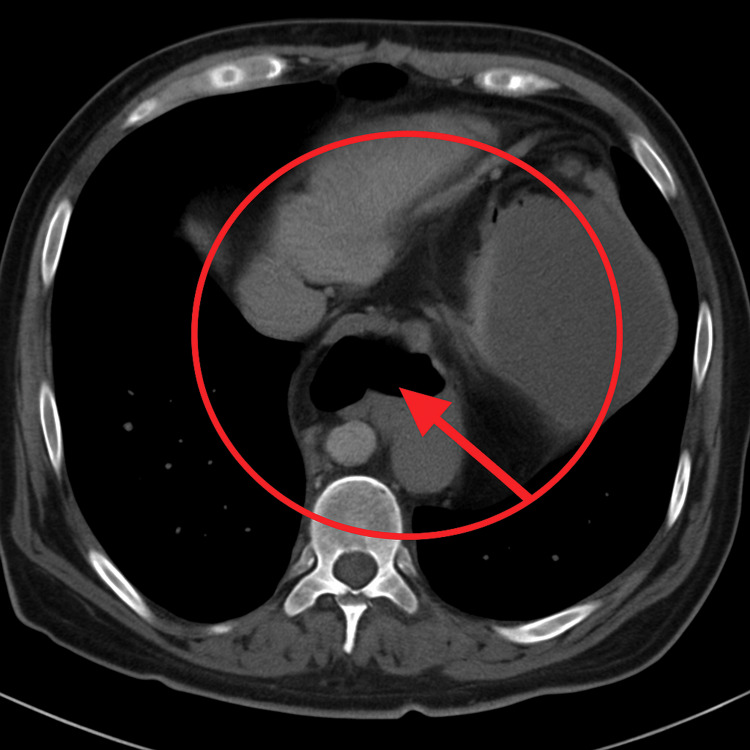
Gastric volvulus is a rare but potentially life-threatening condition that can arise as a complication of a giant hiatal hernia. It results from an abnormal rotation of the stomach, which can lead to obstruction, ischemia, or even gastric necrosis. Prompt recognition and surgical intervention are essential to prevent serious outcomes. We present the case of a 58-year-old female patient with a history of hypertension who arrived at the emergency department with acute-onset severe epigastric pain (10/10 on the Visual Analog Scale), accompanied by nausea but no vomiting. Physical examination revealed involuntary guarding in the epigastric region. Initial imaging with contrast-enhanced esophagogram showed a giant hiatal hernia with intrathoracic migration of the stomach and signs of gastric volvulus. A subsequent computed tomography (CT) scan confirmed the herniation of the gastric antrum through the esophageal hiatus with organoaxial rotation. The patient underwent urgent laparoscopic surgery. Intraoperatively, the stomach was found to be viable, with no evidence of necrosis or perforation. The herniated stomach was reduced, and the esophageal hiatus was dissected and repaired using a prosthetic mesh. The patient had an uneventful postoperative course and was discharged on the second postoperative day. She remains asymptomatic at follow-up. This case highlights the importance of early diagnosis and intervention in patients with acute gastric volvulus, especially when associated with a giant hiatal hernia. Laparoscopic repair remains the gold standard, offering reduced morbidity, faster recovery, and favorable long-term outcomes. A literature review confirms that surgical correction of the anatomical defect is essential to prevent recurrence and severe complications such as ischemia or gastric necrosis. Endoscopic and percutaneous decompression may serve as temporary measures but are not substitutes for definitive surgical treatment.
Keywords: esophagogram; gastric volvulus; giant hiatal hernia; laparoscopic surgery; organoaxial rotation.
Copyright © 2025, Urbina Velázquez et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



Similar articles
-
Gastric volvulus as a rare complication of hiatal hernia: A rare case report.Int J Surg Case Rep. 2025 Aug;133:111582. doi: 10.1016/j.ijscr.2025.111582. Epub 2025 Jun 27. Int J Surg Case Rep. 2025. PMID: 40582065 Free PMC article.
-
Breaking Boundaries: A Case Report of Giant Hiatal Hernia Housing Pancreas, Stomach, Small Bowel, and Colon.Cureus. 2025 Aug 17;17(8):e90317. doi: 10.7759/cureus.90317. eCollection 2025 Aug. Cureus. 2025. PMID: 40843055 Free PMC article.
-
Laparoscopic Management of a Strangulated Hiatal Hernia: A Case Report.Cureus. 2025 May 24;17(5):e84731. doi: 10.7759/cureus.84731. eCollection 2025 May. Cureus. 2025. PMID: 40551911 Free PMC article.
-
Assessing the comparative effects of interventions in COPD: a tutorial on network meta-analysis for clinicians.Respir Res. 2024 Dec 21;25(1):438. doi: 10.1186/s12931-024-03056-x. Respir Res. 2024. PMID: 39709425 Free PMC article. Review.
-
Defining disease severity in atopic dermatitis and psoriasis for the application to biomarker research: an interdisciplinary perspective.Br J Dermatol. 2024 Jun 20;191(1):14-23. doi: 10.1093/bjd/ljae080. Br J Dermatol. 2024. PMID: 38419411 Free PMC article. Review.
References
-
- The threatened stomach: management of the acute gastric volvulus. Light D, Links D, Griffin M. Surg Endosc. 2016;30:1847–1852. - PubMed
-
- Laparoscopic repair of chronic intrathoracic gastric volvulus. Katkhouda N, Mavor E, Achanta K, et al. Surgery. 2000;128:784–790. - PubMed
-
- Acute vs. elective paraesophageal hernia repair: endoscopic gastric decompression allows semi-elective surgery in a majority of acute patients. Wirsching A, El Lakis MA, Mohiuddin K, Pozzi A, Hubka M, Low DE. J Gastrointest Surg. 2018;22:194–202. - PubMed
-
- Use of single percutaneous endoscopic gastrostomy in management of gastric volvulus in three patients. Tsang TK, Johnson YL, Pollack J, Gore RM. Dig Dis Sci. 1998;43:2659–2665. - PubMed
Publication types
LinkOut - more resources
Full Text Sources