

Whipple Disease With Central Nervous System Involvement
- PMID: 40530372
- PMCID: PMC12169642
- DOI: 10.12788/fp.0542
Whipple Disease With Central Nervous System Involvement
Abstract
Background: Whipple disease is a rare, chronic, and systemic infectious disease caused by the bacterium Tropheryma whipplei. It can be mistaken for numerous other diseases, including seronegative rheumatoid arthritis and tropical sprue, and it is known to occur concurrently with giardiasis. Whipple disease can be fatal if not promptly recognized and treated.
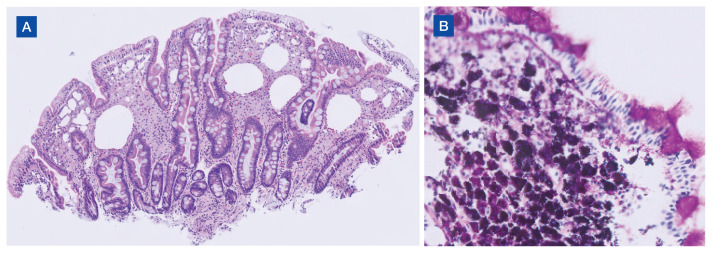
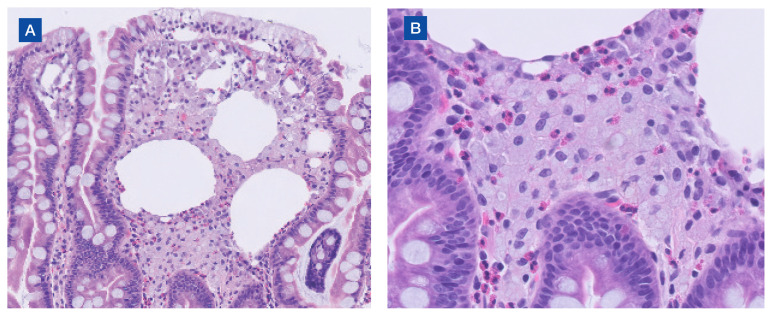
Case presentation: A 53-year-old male presented with an 8-month history of persistent diarrhea, memory distortion, visual disturbances, 30-lb weight loss, and intermittent bilateral hand and knee arthralgias. An autoimmune evaluation for arthralgia was negative. Polymerase chain reaction testing of duodenal biopsy tissue and cerebrospinal fluid was positive for Tropheryma whipplei.
Conclusions: Whipple disease should be considered in the differential diagnosis when patients present with chronic seronegative arthritis, gastrointestinal abnormalities, and cognitive changes. This case, along with others reported in the literature, point to the importance of additional testing for Whipple disease, even when a concurrent infection, such as giardiasis, has been identified.
Copyright © 2024 Frontline Medical Communications Inc., Parsippany, NJ, USA.
Conflict of interest statement
Author disclosures: The authors report no actual or potential conflicts of interest or outside sources of funding with regard to this article.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources