

Treatment outcomes of successful M1 versus M2 thrombectomy for low-ASPECTS stroke patients
- PMID: 40530425
- PMCID: PMC12176791
- DOI: 10.1177/15910199251343283
Treatment outcomes of successful M1 versus M2 thrombectomy for low-ASPECTS stroke patients
Abstract
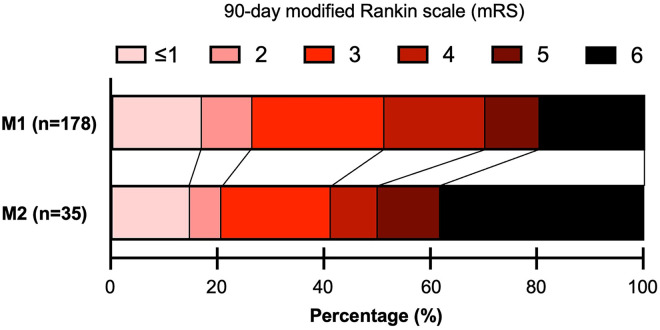
BackgroundThe effectiveness of endovascular thrombectomy (EVT) for low Alberta Stroke Program Early CT score (ASPECTS) stroke patients with occlusion of the second segment of the middle cerebral artery (M2) is unclear.MethodsThis was a multicenter retrospective study. Patients with M1 or M2 occlusions and low ASPECTS (<6) who underwent successful EVT (modified treatment in cerebral ischemia score of 2b or higher) were included. Primary outcome was futile EVT reperfusion (defined as 90-day modified Rankin scale of 5 or 6). Other outcomes of interest include acceptable outcomes (modified Rankin scale of 3 or less) and intracranial hemorrhage (ICH), and all-cause 90-day mortality. Outcomes for M1 patients were compared to M2 patients with multivariable logistic regression models accounting for potential confounders.Results173 patients with M1 or M2 occlusions and low ASPECTS (<6) who underwent successful EVT were identified. After multivariable adjustments, M2 patients had significantly higher odds of futile reperfusion (OR 5.48 [95%CI 1.91 to 15.7], p = 0.002), lower odds of acceptable outcomes (OR 0.33 [95%CI 0.12 to 0.89], p = 0.028), and higher odds of all-cause mortality (OR 4.90 [95%CI 1.65 to 14.5], p = 0.004). These findings suggest that EVT's efficacy for low-ASPECTS stroke patients may be diminished for patients with M2 occlusions. M2 occlusion was not significantly associated with ICH.ConclusionsAmong low-ASEPCTS stroke patients who underwent successful EVT, those with M2 occlusions had significantly higher odds of poor outcome compared to those with M1 occlusions.
Keywords: ASPECTS; M2; Stroke; medium; thrombectomy.
Conflict of interest statement
The STAR registry receives research support from Penumbra, Microvention, Medtronic, Stryker, RapidAI, Brain Aneurysm Foundation. HChen: None. MC: None. HM: None. CC: None. AA: None. DA: Consultant for MicroVention, Stryker, Q'apel, Synchron, and Cerenovus, Investor Von Vascular, Research Support The Bee Foundation. WB: Holds equity in Nested Knowledge, Superior Medical Editors, Piraeus Medical, Sonoris Medical, and MIVI Neurovascular. He receives royalties from Medtronic and Balloon Guide Catheter Technology. He receives consulting fees from Medtronic, Stryker, Imperative Care, Microvention, MIVI Neurovascular, Cerenovus, Asahi, and Balt. He serves in a leadership or fiduciary role for MIVI Neurovascular, Marblehead Medical LLC, Interventional Neuroradiology (Editor in Chief), Piraeus Medical, and WFITN. SC: Consultant and proctor for Medtronic and Microvention. RC: none. HCuellar: Consultant for Medtronic and Microvention. ED: None. RDL: PI for Imperative Trial; Research grants from Siemens Healthineers and Kaneka Medical. Consultant for Cerenovus, Stryker Neurovascular and Sim & Cure. Minor equity interest Vastrax, Borvo medical, Synchron, Endostream, Von Vascular, Radical catheters and Precision Recovery Inc. ME: Consultant for Viz.ai and Imperative Care. Investments in Galaxy Therapeutics. IF: None. NG: None. RG: Consultant for Balt Neurovascular, Cerenovus, Medtronic Neurovascular, Rapid Medical, and Stryker Neurovascular. BH: None. PJ: None. PK: Grants from the NIH (1U18EB029353-01) and unrestricted educational grants from Medtronic and Siemens. Consultant for Imperative Care and Stryker Neurovascular. Stock ownership in Vena Medical. JTK: None. MRL: Unrestricted educational grants from Medtronic and Stryker; consulting agreement with Medtronic, Aeaean Advisers and Metis Innovative; equity interest in Proprio, Stroke Diagnostics, Apertur, Stereotaxis, Fluid Biomed, and Hyperion Surgical; editorial board of Journal of NeuroInterventional Surgery; Data safety monitoring board of Arsenal Medical. IM: speakers honoraria from Pfizer and Bristol-Myers Squibb. JM: None. CM: Consultant for Stryker, Medtronic, Microvention, Penumbra, and Silk Road Medical. Speaker for Penumbra and Silk Road Medical. Contact PI for NIH Grant R21NS128641. MM: None. PN: Consultant for Penumbra, Medtronic, Stryker, Cerenovus and Balt. JO: None. MSP: Consultant for Medtronic. AP: None: MNP: Grants from the Swiss National Science Foundation (SNF) for the DISTAL trial (33IC30_198783) and TECNO trial (32003B_204977), Grant from Bangerter-Rhyner Stiftung for the DISTAL trial. Unrestricted Grants for the DISTAL trial from Stryker Neurovascular Inc., Phenox GmbH, Penumbra Inc. and Rapid Medical Inc., Sponsor-PI SPINNERS trial (Funded by a Siemens Healthineers AG Grant), Research agreement with Siemens Healthineers AG, Local PI for the ASSIST, EXCELLENT, TENSION, COATING, SURF and ESCAPE-NEXT trials. Speaker fees: Stryker Neurovascular Inc., Medtronic Inc., Penumbra Inc., Acandis GmbH, Phenox GmbH, Siemens Healthineers AG. AR: None. DR: Consultant for Penumbra, Balt, Microvention, Phenox. AShaban: None. ASpiotta: Consultant for Penumbra, Terumo, RapidAI, Cerenovus. RS: RMS research is supported by the NREF, Joe Niekro Foundation, Brain Aneurysm Foundation, Bee Foundation, Department of Health Biomedical Research Grant (21K02AWD-007000) and by National Institute of Health (R01NS111119-01A1) and (UL1TR002736, KL2TR002737) through the Miami Clinical and Translational Science Institute, from the National Center for Advancing Translational Sciences and the National Institute on Minority Health and Health Disparities. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. RMS has an unrestricted research grant from Medtronic and Balt and has consulting and teaching agreements with Penumbra, Abbott, Medtronic, Balt, InNeuroCo, Cerenovus, Naglreiter, Tonbridge, Von Medical, and Optimize Vascular. OT: Consulting Agreements: Viz.AI, Inc., Penumbra, Inc, Balt, Inc, Stryker Inc, Imperative Inc. Proctor: Microvention Inc, Medtronic Inc. Educational/Research Grants: Q’apel Inc, Steinberg Foundation. RW: Consultant for Medtronic, Stryker, and Synaptive Medical. SQW: None. SY: lecture fee from Stryker, Medtronic, Johnson & Johnson, Kaneka Medics. AE: None. AA: Consultant for Cerenovus
Figures
References
-
- Barber PA, Demchuk AM, Zhang Jet al. et al. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS study group. Alberta stroke programme early CT score. Lancet 2000; 355: 1670–1674. - PubMed
-
- Chen H, Colasurdo M. Endovascular thrombectomy for large ischemic strokes: meta-analysis of six multicenter randomized controlled trials. J Neurointerv Surg 2024. jnis-2023-021366. - PubMed
-
- Bendszus M, Fiehler J, Subtil F, et al. Endovascular thrombectomy for acute ischaemic stroke with established large infarct: multicentre, open-label, randomised trial. Lancet 2023; 402: 1753–1763. - PubMed
-
- Yoshimura S, Sakai N, Yamagami H, et al. Endovascular therapy for acute stroke with a large ischemic region. N Engl J Med 2022; 386: 1303–1313. - PubMed
-
- Sarraj A, Hassan AE, Abraham MG, et al. Trial of endovascular thrombectomy for large ischemic strokes. N Engl J Med 2023; 388: 1259–1271. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
