

Outcomes Following Transoral Laser Microsurgery for T1b and T2a Glottic Squamous Cell Carcinoma With and Without Anterior Commissure Involvement: A Retrospective Chart Review
- PMID: 40530452
- PMCID: PMC12177246
- DOI: 10.1177/19160216251348424
Outcomes Following Transoral Laser Microsurgery for T1b and T2a Glottic Squamous Cell Carcinoma With and Without Anterior Commissure Involvement: A Retrospective Chart Review
Abstract
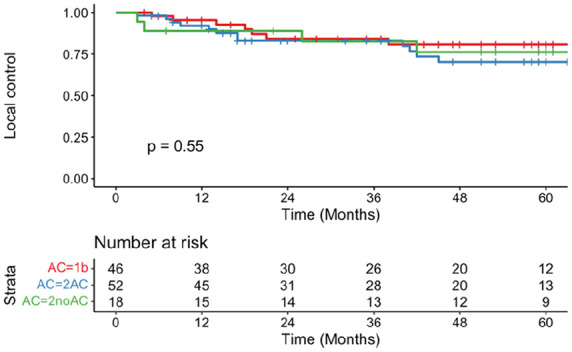
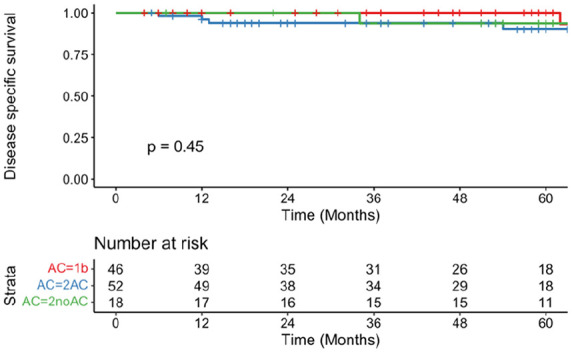
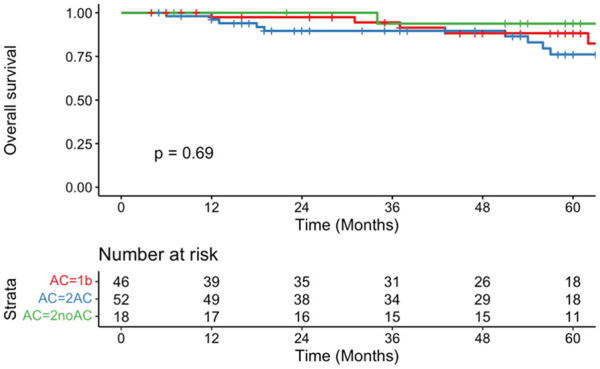
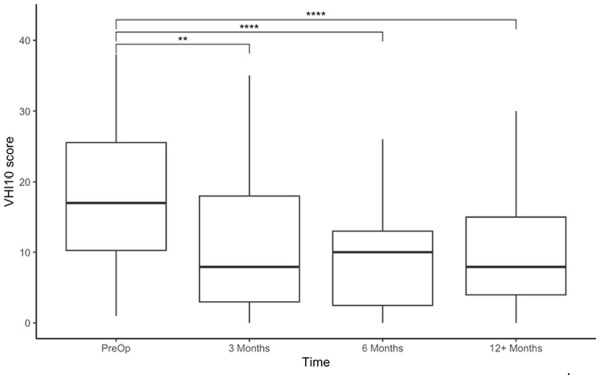
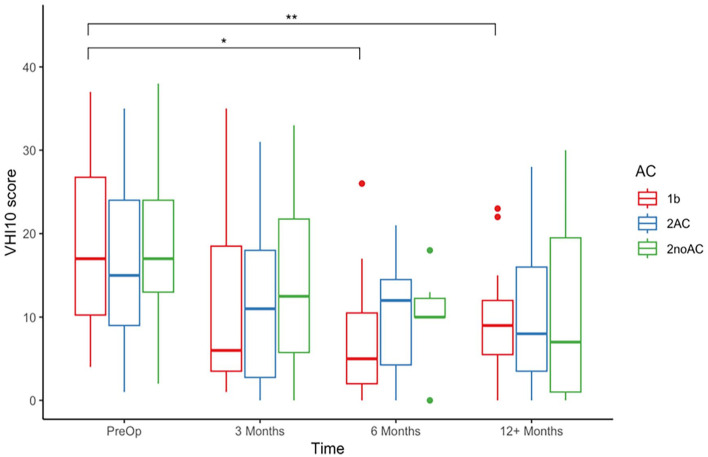
ImportanceThere is a limited understanding of anterior commissure (AC) involvement in glottic squamous cell carcinoma (SCC), particularly when comparing T1b, T2a with AC involvement (T2AC), and T2a without AC involvement (T2noAC).ObjectiveThe aim of this study was to compare oncological and functional outcomes in T1b, T2AC, and T2noAC glottic SCC following transoral laser microsurgery (TLM).DesignRetrospective chart review.SettingThe Queen Elizabeth II Health Science Centre (Halifax, Nova Scotia) from January 1, 2002, to December 31, 2022.Intervention and ExposuresA retrospective chart review was completed using prospectively-collected data for patients treated with TLM for T1b and T2a glottic SCC. Exclusion criteria included previous treatment for a laryngeal cancer and T2b glottic SCC.Main Outcome MeasuresOncological outcomes were assessed using margin status, local control (LC), disease-specific survival (DSS), overall survival (OS), and laryngeal preservation (LP). Functional outcomes were measured using the abbreviated Voice Handicap Index-10 (VHI-10).ResultsIn total, 117 patients were included (T1b = 46, T2AC = 53, T2noAC = 18). Positive margins were higher in the T2AC group (15.1%) than in T1b (4.3%) and T2noAC (5.6%; P = .208). At 5 years, there were no significant differences in LC (T1b = 80.8%, T2AC = 70.3%, T2noAC = 76.2%; P = .26), DSS (T1b = 100%, T2AC = 90.2%, T2noAC = 93.8%; P = .45), OS (T1b = 88.3%, T2AC = 76.1%, T2noAC = 93.8%; P = .69), or LP (T1b = 94.3%, T2AC = 92.1%, T2noAC = 94.4%; P = .74). Significant improvements in VHI-10 scores from the pre- to postoperative period were only noted in the T1b cohort, at the 6 months (P = .017) and the 12 months (P = .00143).ConclusionsNo significant differences in both oncological and functional outcomes were noted between T1b, T2AC, and T2noAC glottic SCCs. Further stratifying based on the degree and pattern of AC involvement with larger sample sizes may provide important prognostic factors.RelevanceThis study highlights that T2 glottic SCCs with normal vocal fold mobility are a heterogenous group, and it may be beneficial to further stratify these cancers according to AC involvement, particularly when considering TLM.
Keywords: glottic cancer; laryngeal cancer; transoral laser microsurgery.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Transoral laser microsurgery versus radiotherapy for T2 glottic squamous cell carcinoma: a systematic review of local control outcomes.Clin Otolaryngol. 2017 Jun;42(3):629-636. doi: 10.1111/coa.12790. Epub 2016 Dec 4. Clin Otolaryngol. 2017. PMID: 27863075
-
Therapeutic modalities and oncologic outcomes in the treatment of T1b glottic squamous cell carcinoma: a systematic review.Eur Arch Otorhinolaryngol. 2017 Dec;274(12):4091-4102. doi: 10.1007/s00405-017-4736-z. Epub 2017 Sep 19. Eur Arch Otorhinolaryngol. 2017. PMID: 28929221
-
Oncologic and functional outcomes of patients treated with transoral CO2 laser microsurgery or radiotherapy for T2 glottic carcinoma: a systematic review of the literature.Curr Opin Otolaryngol Head Neck Surg. 2018 Apr;26(2):84-93. doi: 10.1097/MOO.0000000000000438. Curr Opin Otolaryngol Head Neck Surg. 2018. PMID: 29278552
-
Transoral Laser Microsurgery Versus Radiotherapy for T1-T2 Glottic Cancer with Anterior Commissure Involvement: A Systematic Review and Meta-Analysis.Laryngoscope. 2025 Jun;135(6):1861-1871. doi: 10.1002/lary.32005. Epub 2025 Jan 11. Laryngoscope. 2025. PMID: 39797764
-
Radiotherapy or surgical treatment of early glottic carcinoma: A population-based study from the Swedish Head and Neck Cancer Register evaluating primary treatment outcomes for patients with T1a/T1b tumors.Cancer. 2025 Jul 1;131(13):e35955. doi: 10.1002/cncr.35955. Cancer. 2025. PMID: 40569651 Free PMC article.
References
-
- Rucci L, Gammarota L, Borghi Cirri MB. Carcinoma of the anterior commissure of the larynx: I. Embryological and anatomic considerations. Ann Otol Rhinol Laryngol. 1996;105:303-308. - PubMed
-
- Bagatella F, Bignardi L. Morphological study of the laryngeal anterior commissure with regard to the spread of cancer. Acta Otolaryngol. 1981;92:167-171. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
