

Risk of Death, Infections, and Hyperthermia in Ectodermal Dysplasias: A Nationwide Study
- PMID: 40530795
- PMCID: PMC12186435
- DOI: 10.2340/actadv.v105.43101
Risk of Death, Infections, and Hyperthermia in Ectodermal Dysplasias: A Nationwide Study
Abstract
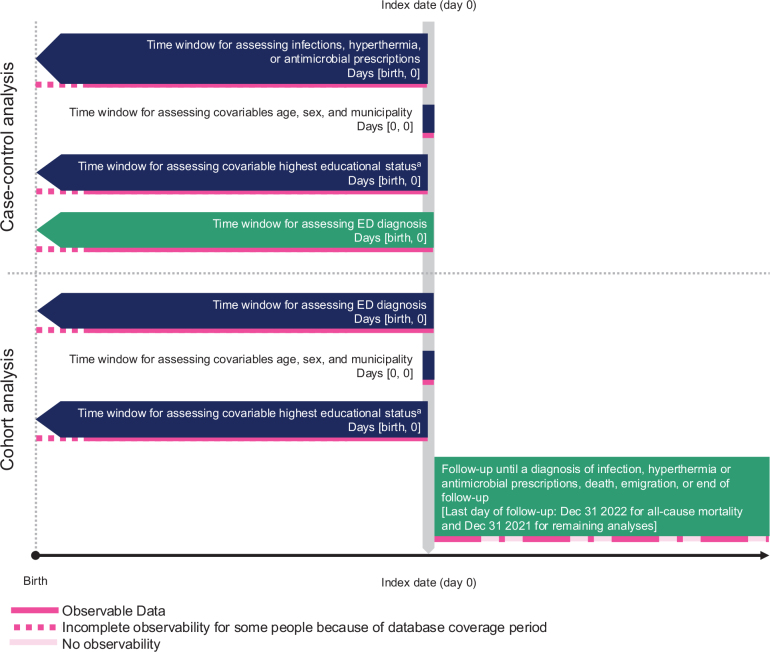
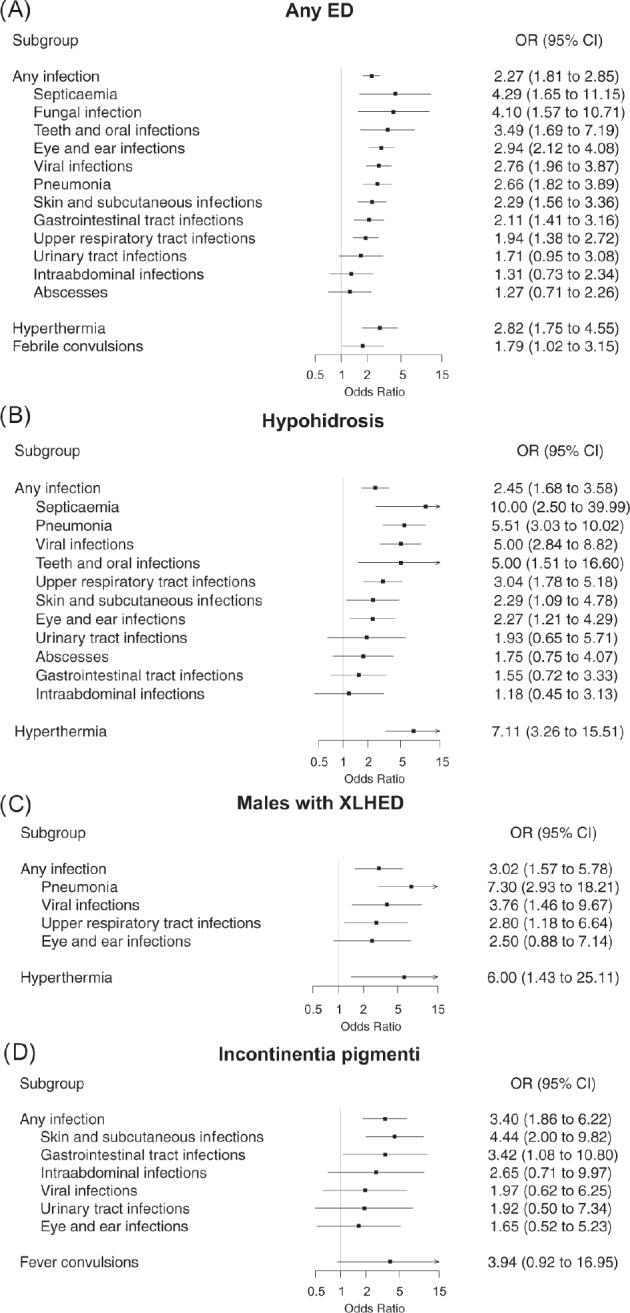
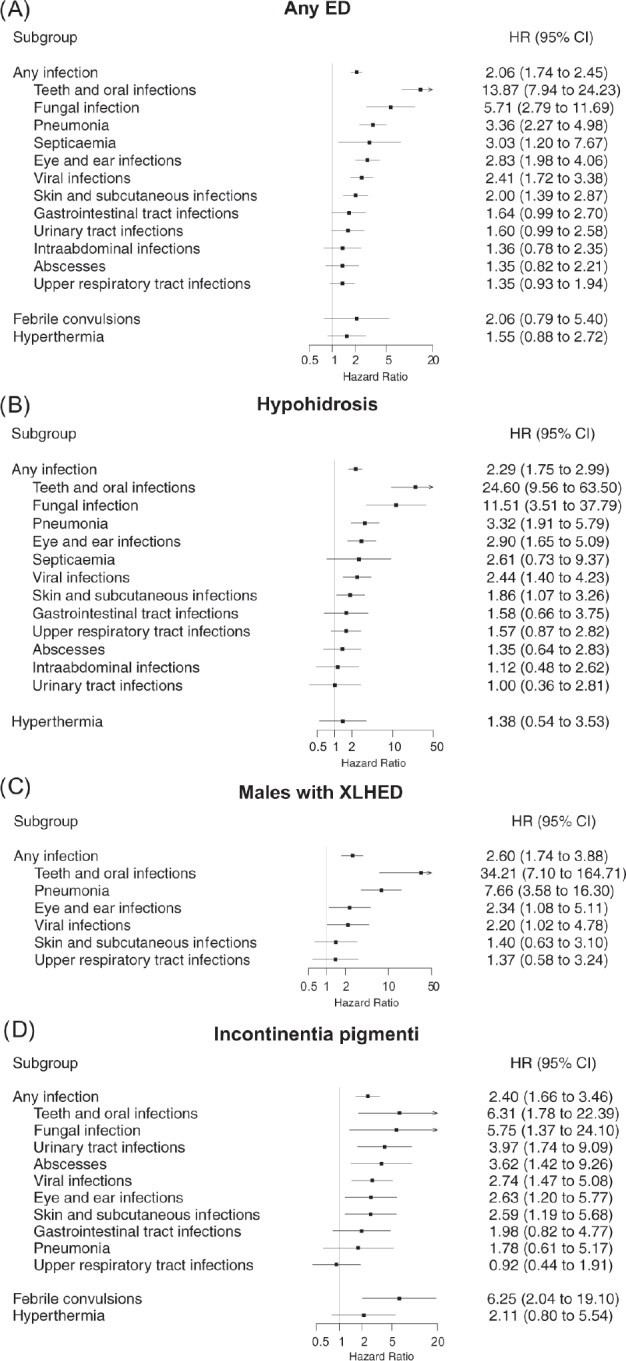
This nationwide population-based study investigated the risk of death, infections, and hyperthermia in Danish patients with ectodermal dysplasia (ED). A validated cohort of ED patients (n = 396) and matched population comparators (n = 3960) was compared to assess these risks before (case-control analysis) and after ED diagnosis (cohort analysis). Using matched comparators as a reference, the overall hazard ratio (HR) for death was 1.33 (95% confidence interval [CI] 0.70-2.55) in ED patients, and particularly high in males with hypohidrosis (HR 3.77, 95% CI 1.57-9.03) and individuals diagnosed before age 18 (HR 6.53, 95% CI 1.84-23.13). ED was associated with an increased risk of hospital-diagnosed infections before (odds ratio [OR] 2.27, 95% CI 1.81-2.85) and after (HR 2.06, 95% CI 1.74-2.45) diagnosis, varying across subtypes. Sensitivity analyses supported these findings, e.g., using antimicrobial prescriptions to identify infections. An association between hypohidrosis and previous hyperthermia (OR 7.11, 95% CI 3.26-15.51) diminished after diagnosis (HR 1.38, 95% CI 0.54-3.53). This study found an increased mortality risk in males with hypohidrosis and those diagnosed in childhood, and infection and hyperthermia risks depending on ED subtype. These data enhance understanding of ED's clinical course, informing patient management and counselling.
Conflict of interest statement
Sigrún A.J. Schmidt has received speaker honoraria from GSK Pharma for lectures unrelated to the present study. Mette Sommerlund received honoraria from Leo-Pharma and Sanofi for lectures unrelated to the present study. Laura Krogh Herlin and Trine H. Mogensen have no conflicts of interest to disclose.
Figures
Similar articles
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Repeat doses of prenatal corticosteroids for women at risk of preterm birth for improving neonatal health outcomes.Cochrane Database Syst Rev. 2022 Apr 4;4(4):CD003935. doi: 10.1002/14651858.CD003935.pub5. Cochrane Database Syst Rev. 2022. PMID: 35377461 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
References
-
- Fete TJ, Grange DK. Ectodermal dysplasias. In: UpToDate, Connor RF (Ed), Wolters Kluwer. [Accessed on May 5, 2023]
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
