

Framework for Brain-Derived Dimensions of Psychopathology
- PMID: 40531512
- PMCID: PMC12177734
- DOI: 10.1001/jamapsychiatry.2025.1246
Framework for Brain-Derived Dimensions of Psychopathology
Abstract
Importance: Psychiatric diagnoses are not defined by neurobiological measures hindering the development of therapies targeting mechanisms underlying mental illness. Research confined to diagnostic boundaries yields heterogeneous biological results, whereas transdiagnostic studies often investigate individual symptoms in isolation.
Objective: To develop a framework that groups clinical symptoms compatible with ICD-10 and DSM-5 according to their covariation and shared brain mechanisms.
Design, setting, and participants: This diagnostic study was conducted in 2 samples, the population-based Reinforcement-Related Behaviour in Normal Brain Function and Psychopathology (IMAGEN) cohort (longitudinal assessments at 14, 19, and 23 years; study duration from March 2010 to the present) and the cross-diagnostic Brain Network Based Stratification of Mental Illness (STRATIFY)/Earlier Detection and Stratification of Eating Disorders and Comorbid Mental Illnesses (ESTRA) samples (study duration from October 2016 to September 2023). The samples are from 8 clinical research hospitals in Germany, the UK, France, and Ireland. For the population-based IMAGEN study, 794 of 1253 23-year-old participants had complete assessments including complete clinical assessments and neuroimaging data across all time points. For the cross-diagnostic STRATIFY/ESTRA samples, 209 of 485 participants aged 18 to 26 years had complete clinical and neuroimaging data. The sample included healthy control individuals and patients with alcohol use disorder, major depressive disorder, anorexia nervosa, and bulimia nervosa.
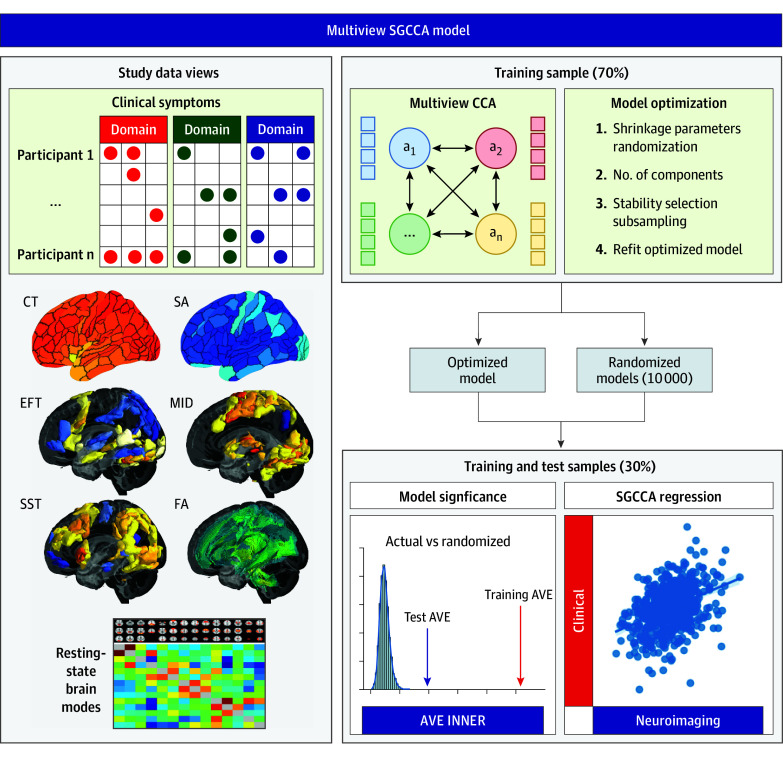
Exposures: Sparse generalized canonical correlation analysis was used to integrate diverse data from clinical symptoms and 7 brain imaging modalities.
Main outcomes and measures: The prediction of symptom features was the main outcome. The model was developed in the training set from the IMAGEN Study at age 23 years (70%), then applied in the remaining holdout test sample (30%), the independent STRATIFY/ESTRA patient sample, and longitudinally in the IMAGEN set.
Results: In total, 1003 participants were included (425 male and 578 female; mean [SD] age, 22.1 [1.5] years). The reassembly of existing ICD-10 and DSM-5 symptoms revealed 6 cross-diagnostic psychopathology scores. They were consistently associated with multimodal neuroimaging components: excitability and impulsivity (training set: r, 0.26; 95% CI, 0.18-0.33; test set: r, 0.22; 95% CI, 0.10-0.35; STRATIFY/ESTRA set: r, 0.19; 95% CI, 0.07-0.31), depressive mood and distress (training: r, 0.30; 95% CI, 0.20-0.38; test: r, 0.22; 95% CI, 0.09-0.35; STRATIFY/ESTRA: r, 0.19; 95% CI, 0.04-0.33), emotional and behavioral dysregulation (training: r, 0.40; 95% CI, 0.31-0.48; test: r, 0.17; 95% CI, 0.14-0.36; STRATIFY/ESTRA: r, 0.19; 95% CI, 0.06-0.30), stress pathology (training: r, 0.32; 95% CI, 0.19-0.43; test: r, 0.14; 95% CI, 0.05-0.23; STRATIFY/ESTRA: r, 0.12; 95% CI, 0.01-0.22), eating pathology (training: r, 0.34; 95% CI, 0.25-0.42; test: r, 0.26; 95% CI, 0.15-0.37; STRATIFY/ESTRA: r, 0.15; 95% CI, 0.12-0.34), and social fear and avoidance symptoms (training: r, 0.31; 95% CI, 0.25-0.42; test: r, 0.18; 95% CI, 0.15-0.35; STRATIFY/ESTRA: r, 0.12; 95% CI, 0.12-0.33).
Conclusion and relevance: In this study, the identification of symptom groups of mental illness robustly defined by precisely characterized brain mechanisms enabled the characterization of dimensions of psychopathology based on quantifiable neurobiological measures.
Conflict of interest statement
Figures




References
-
- Opel N, Goltermann J, Hermesdorf M, Berger K, Baune BT, Dannlowski U. Cross-disorder analysis of brain structural abnormalities in six major psychiatric disorders: a secondary analysis of mega- and meta-analytical findings from the ENIGMA Consortium. Biol Psychiatry. 2020;88(9):678-686. doi: 10.1016/j.biopsych.2020.04.027 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
