

Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: systematic review and network meta-analysis of randomised clinical trials
- PMID: 40533200
- PMCID: PMC12175170
- DOI: 10.1136/bmj-2024-082007
Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: systematic review and network meta-analysis of randomised clinical trials
Erratum in
-
Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: systematic review and network meta-analysis of randomised clinical trials.BMJ. 2025 Aug 18;390:r1737. doi: 10.1136/bmj.r1737. BMJ. 2025. PMID: 40825602 Free PMC article. No abstract available.
Abstract
Objective: To assess the effect of intermittent fasting diets, with continuous energy restriction or unrestricted (ad-libitum) diets on intermediate cardiometabolic outcomes from randomised clinical trials.
Design: Systematic review and network meta-analysis.
Data sources: Medline, Embase, and central databases from inception to 14 November 2024.
Eligibility criteria for selecting studies: Randomised clinical trials comparing the association of intermittent fasting diets (alternate day fasting, time restricted eating, and whole day fasting), continuous energy restriction, and ad-libitum diets were included.
Main outcomes: Outcomes included body weight (primary) and measures of anthropometry, glucose metabolism, lipid profiles, blood pressure, C-reactive protein, and markers of liver disease.
Data synthesis: A network meta-analysis based on a frequentist framework was performed with data expressed as mean difference with 95% confidence intervals (CIs). The certainty of the evidence was assessed using grading of recommendations assessment, development, and evaluation (GRADE).
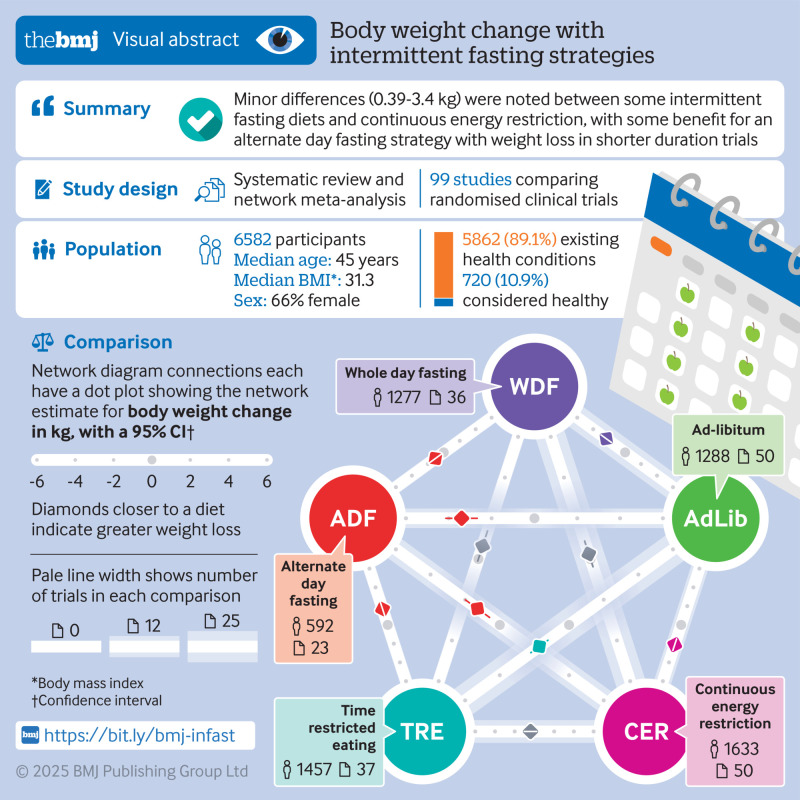
Results: 99 randomised clinical trials involving 6582 adults of varying health conditions (720 healthy, 5862 existing health conditions) were identified. All intermittent fasting and continuous energy restriction diet strategies reduced body weight when compared with ad-libitum diet. Compared with continuous energy restriction, alternate day fasting was the only form of intermittent fasting diet strategy to show benefit in body weight reduction (mean difference -1.29 kg (95% CI -1.99 to -0.59), moderate certainty of evidence). Additionally, alternate day fasting showed a trivial reduction in body weight compared with both time restricted eating and whole day fasting (mean difference -1.69 kg (-2.49 to -0.88) and -1.05 kg (-1.90 to -0.19), respectively, both with moderate certainty of evidence). Estimates were similar among trials with less than 24 weeks follow-up (n=76); however, moderate-to-long-term trials (≥24 weeks, n=17) only showed benefits in weight reduction in diet strategies compared with ad-libitum. Furthermore, in comparisons between intermittent fasting strategies, alternate day fasting lowered total cholesterol, triglycerides, and non-high density lipoprotein compared with time restricted eating. Compared with whole day fasting, however, time restricted eating resulted in a small increase in total cholesterol, low density lipoprotein cholesterol, and non-high density lipoprotein cholesterol. No differences were noted between intermittent fasting, continuous energy restriction, and ad-libitum diets for HbA1c and high density lipoprotein.
Conclusions: Minor differences were noted between some intermittent fasting diets and continuous energy restriction, with some benefit of weight loss with alternate day fasting in shorter duration trials. The current evidence provides some indication that intermittent fasting diets have similar benefits to continuous energy restriction for weight loss and cardiometabolic risk factors. Longer duration trials are needed to further substantiate these findings.
Trial registration: ClinicalTrials.gov NCT05309057.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: TAK has received research support from the CIHR, the International Life Science Institute and National Honey Board. He has been an invited speaker at the Calorie Control Council Annual meeting for which he has received an honorarium. LC held a Mitacs-Elevate post-doctoral fellowship jointly funded by the Government of Canada and the Canadian Sugar Institute (2019-2021). She was employed as a casual clinical coordinator at INQUIS Clinical Research, Ltd. (formerly Glycemic Index Laboratories, Inc), a contract research organization (until 2019). She has received research funding from the Canadian Institutes of Health Research (CIHR), Protein Industries Canada (a Government of Canada Global Innovation Cluster), the United Soybean Board (The United States Department of Agriculture Soybean “Check-off” Program), and the Alberta Pulse Growers. She has received honoraria from the Arkansas Children’s Hospital and travel funding from the World Sugars Research Organization for an internal presentation in 2022. SK received grants by the German Center for Diabetes Research (DZD), the German Diabetes Association, the Almond Board of California, the California Walnut Commission, the Wilhelm-Doerenkamp-Foundation. DCWL reports clinical research grant funding from Novo Nordisk. He serves on advisory boards for Amgen, Bayer, Boehringer Ingelheim, HLS Therapeutics, Eli Lilly, Novartis, Novo Nordisk, Pfizer, and Viatris. He serves on speaker bureaus for Amgen, Bayer, Boehringer Ingelheim, CME at Sea, HLS Therapeutics, Eli Lilly, Novartis, Novo Nordisk, and Obesity Canada. He is the founder of Obesity Canada and a member of the board of directors of Canadian Association of Bariatric Physicians and Surgeons for no remuneration. JOH reports speaker fees from Eli Lilly. He serves as a member of the scientific advisory board for General Mills. ML reports membership of the Arctic Clum and the Alpine Club, departmental research support from National Institute for Health Research (NIHR), Novo Nordisk Diabetes UK, and All Saints Educational Trust, outside the submitted work, lecturing fees from Novo Nordisk, Eli Lilly, Nestle, and Oviva, and has provided clinical consultancy to the Government of Bermuda, the Ombudsman of Northern Ireland, and Counterweight Ltd, with fees paid to the University of Glasgow. SW has been involved in honoraria, ad boards, or clinical trials for Novo Nordisk Inc, Bausch Health Canada, Eli Lilly, and Boehringer Engelheim. DR is director of Vuk Vrhovac University Clinic for Diabetes, Endocrinology and Metabolic Diseases at Merkur University Hospital, Zagreb, Croatia. He is the president of Croatian Society for Diabetes and Metabolic Disorders of Croatian Medical Association. He serves as an executive committee member of Croatian Endocrine Society, Croatian Society for Obesity and Croatian Society for Endocrine Oncology. He was a board member and secretary of International Diabetes Federation (IDF) Europe and currently he is the chair of the IDF Young Leaders in Diabetes Programme. He has served as an executive committee member of the Diabetes and Nutrition Study Group of European Association of the Study of Diabetes (EASD) and currently he serves as an executive committee member of Diabetes and Cardiovascular Disease Study Group of EASD. He has served as principal investigator or coinvestigator in clinical trials of AstraZeneca, Eli Lilly, MSD, Novo Nordisk, Sanofi Aventis, Solvay, and Trophos. He has received travel support, speaker fees, and honoraria from advisory board engagements and consulting fees from Abbott, Amgen, AstraZeneca, Bayer, Belupo, Boehringer Ingelheim, Eli Lilly, Lifescan – Johnson and Johnson, International Sweeteners Association, Krka, Medtronic, Mediligo, Mylan, Novartis, Novo Nordisk, MSD, Merck Sharp and Dohme, Pfizer, Pliva, Roche, Salvus, Sandoz, Solvay, Sanofi Aventis, and Takeda. JS-S is on the Clinical Practice Guidelines Expert Committee of EASD and served in the Scientific Committee of the Spanish Food and Safety Agency and the Spanish Federation of the Scientific Societies of Food, Nutrition and Dietetics. He is a member of the International Carbohydrate Quality Consortium (ICQC) and Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD, and has received research support from the Instituto de Salud Carlos III, Spain, Ministerio de Educación y Ciencia, Spain, Departament de Salut Pública de la Generalitat de Catalunya, Catalonia, Spain, and the European Commission. Reported receiving personal fees from Instituto Danone Spain. Received financial support to the institution from the International Nut and Dried Fruit Council Foundation, Fundación Eroski. He is a non-paid member of the International Danone Institute and received travel expenses form this institution. CWCK has received grants or research support from the Advanced Food Materials Network, Agriculture and Agri-Foods Canada (AAFC), Almond Board of California, Barilla, Canadian Institutes of Health Research (CIHR), Canola Council of Canada, International Nut and Dried Fruit Council, International Tree Nut Council Research and Education Foundation, Loblaw Brands Ltd, the Peanut Institute, Pulse Canada, and Unilever. He has received in-kind research support from the Almond Board of California, Barilla, California Walnut Commission, Kellogg Canada, Loblaw Companies, Nutrartis, Quaker (PepsiCo), the Peanut Institute, Primo, Unico, Unilever, and WhiteWave Foods/Danone. He has received travel support and/or honoraria from the Barilla, California Walnut Commission, Canola Council of Canada, General Mills, International Nut and Dried Fruit Council, International Pasta Organization, Lantmannen, Loblaw Brands Ltd, Nutrition Foundation of Italy, Oldways Preservation Trust, Paramount Farms, the Peanut Institute, Pulse Canada, Sun-Maid, Tate & Lyle, Unilever, and White Wave Foods/Danone. He has served on the scientific advisory board for the International Tree Nut Council, International Pasta Organization, McCormick Science Institute, and Oldways Preservation Trust. He is a founding member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the DNSG of the EASD, is on the Clinical Practice Guidelines Expert Committee for Nutrition Therapy of the EASD and is a Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. JLS has received research support from the Canadian Foundation for Innovation, Ontario Research Fund, Province of Ontario Ministry of Research and Innovation and Science, Canadian Institutes of health Research (CIHR), Diabetes Canada, American Society for Nutrition (ASN), National Honey Board (U.S. Department of Agriculture (USDA) honey “Checkoff” program), Institute for the Advancement of Food and Nutrition Sciences (IAFNS), Pulse Canada, Quaker Oats Center of Excellence, INC International Nut and Dried Fruit Council Foundation, The United Soybean Board (USDA soy “Checkoff” program), Protein Industries Canada (a Government of Canada Global Innovation Cluster), Almond Board of California, European Fruit Juice Association, The Tate and Lyle Nutritional Research Fund at the University of Toronto, The Glycemic Control and Cardiovascular Disease in Type 2 Diabetes Fund at the University of Toronto (a fund established by the Alberta Pulse Growers), The Plant Protein Fund at the University of Toronto (a fund which has received contributions from IFF among other donors), The Plant Milk Fund at the University of Toronto (a fund established by the Karuna Foundation through Vegan Grants), and The Nutrition Trialists Network Fund at the University of Toronto (a fund established by donations from the Calorie Control Council, Physicians Committee for Responsible Medicine, and Login5 Foundation). He has received food donations to support randomised controlled trials from the Almond Board of California, California Walnut Commission, Danone, Nutrartis, Soylent, and Dairy Farmers of Canada. He has received travel support, speaker fees and/or honoraria from FoodMinds LLC, Nestlé, Abbott, General Mills, Nutrition Communications, International Food Information Council (IFIC), Arab Beverage Association, International Sweeteners Association, Calorie Control Council, Phynova, and Collaborative CME and Research Network (CCRN). He has or has had ad hoc consulting arrangements with Almond Board of California, Perkins Coie LLP, Tate & Lyle, Ingredion, and Brightseed. He is on the Clinical Practice Guidelines Expert Committees of Diabetes Canada, EASD, Canadian Cardiovascular Society (CCS), and Obesity Canada/Canadian Association of Bariatric Physicians and Surgeons. He serves as an unpaid member of the Board of Trustees of IAFNS. He is a Director at Large of the Canadian Nutrition Society (CNS), founding member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the DNSG of the EASD, and Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. His spouse is a former employee of Nestle Health Science and AB InBev; no other relationships or activities that could appear to have influenced the submitted work. All other authors declare that they have no competing interests.
Figures





References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous