

Echogenicity of carotid plaques as a predictor of regression following lipid-lowering therapy
- PMID: 40533742
- PMCID: PMC12175450
- DOI: 10.1186/s12959-025-00753-5
Echogenicity of carotid plaques as a predictor of regression following lipid-lowering therapy
Abstract
Objective: Atherosclerotic plaque regression under lipid-lowering therapy shows considerable individual variation, and the factors influencing this variability remain incompletely understood. This study aimed to investigate the relationship between carotid plaque echogenicity and plaque regression in patients receiving lipid-lowering therapy, and to identify ultrasound characteristics that might predict plaque regression.
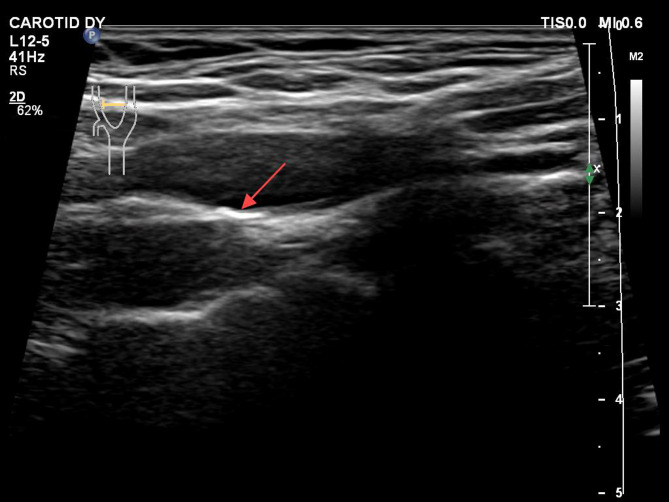
Methods: A total of 838 patients with carotid plaques receiving lipid-lowering therapy were enrolled between July 2020 and May 2024 and followed up for 12 months. Carotid ultrasound was performed at baseline and follow-up to evaluate plaque characteristics. Plaque regression was defined as meeting any of the following criteria: (1) reduction in plaque area ≥ 5%, (2) decrease in plaque thickness ≥ 0.4 mm, or (3) reduction in plaque number, as assessed by vascular ultrasound imaging. Plaque echogenicity was classified into three types: hypoechoic, hyperechoic, and mixed echogenicity. Cox proportional hazards regression analysis was performed to assess the association between plaque echogenicity and plaque regression, adjusting for potential confounding factors.
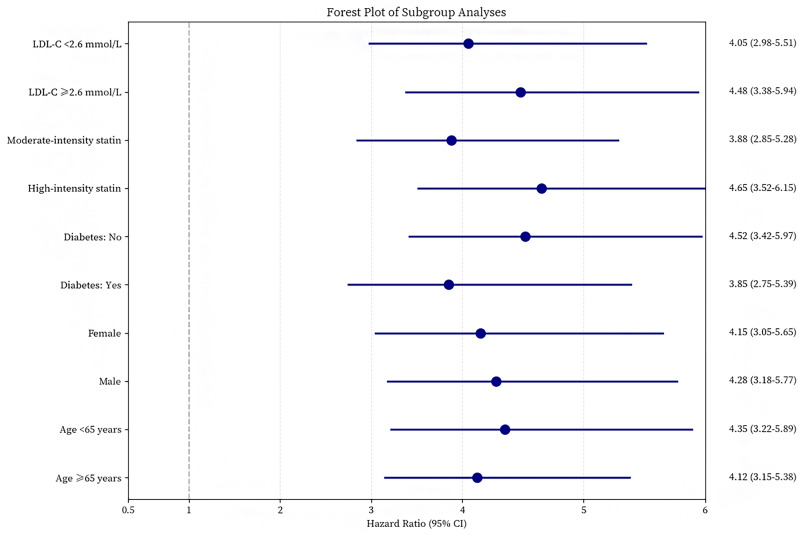
Results: Hypoechoic plaques showed higher rates of regression (72.8%) compared to hyperechoic (37.7%) and mixed echogenicity plaques (50.0%) (p < 0.001). After adjusting for confounding variables, hypoechoic plaques exhibited greater odds of regression compared to hyperechoic plaques (adjusted HR = 4.52, 95% CI: 3.18-6.43, p < 0.001). Additionally, the median percentage reduction in plaque size was more pronounced in hypoechoic plaques, (15.2%, IQR: 7.7-22.3%) compared with other echogenicities (p < 0.001).
Conclusion: Carotid plaque echogenicity is strongly associated with the likelihood plaque regression, with hypoechoic plaques exhibiting higher regression rates and greater reductions in plaque size. These findings may help guide personalized treatment strategies and improve risk assessment.
Keywords: Atherosclerosis; Carotid ultrasound; Echogenicity; Plaque regression.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures





Similar articles
-
Carotid plaque echogenicity predicts cerebrovascular symptoms: a systematic review and meta-analysis.Eur J Neurol. 2016 Jul;23(7):1241-7. doi: 10.1111/ene.13017. Epub 2016 Apr 23. Eur J Neurol. 2016. PMID: 27106563
-
Automated scheme of plaque classification based on segmentation in carotid ultrasound images using transformer approach.J Med Ultrason (2001). 2025 Jul;52(3):271-282. doi: 10.1007/s10396-025-01522-7. Epub 2025 Apr 17. J Med Ultrason (2001). 2025. PMID: 40244313
-
High Risk of Venous Thromboembolism With Aspirin Prophylaxis After THA for High-riding Developmental Dysplasia of the Hip: A Retrospective, Comparative Study.Clin Orthop Relat Res. 2025 Jun 9. doi: 10.1097/CORR.0000000000003482. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40536765
-
Carotid Intraplaque neovascularization correlates with coronary atherosclerotic plaque, vulnerability detected by intracoronary optical coherence tomography.Int J Cardiol. 2025 Oct 15;437:133495. doi: 10.1016/j.ijcard.2025.133495. Epub 2025 Jun 11. Int J Cardiol. 2025. PMID: 40513674
-
Pharmacological and electronic cigarette interventions for smoking cessation in adults: component network meta-analyses.Cochrane Database Syst Rev. 2023 Sep 12;9(9):CD015226. doi: 10.1002/14651858.CD015226.pub2. Cochrane Database Syst Rev. 2023. PMID: 37696529 Free PMC article.
References
-
- Kakkos SK, Griffin MB, Nicolaides AN, et al. The size of juxtaluminal hypoechoic area in ultrasound images of asymptomatic carotid plaques predicts the occurrence of stroke. J Vasc Surg. 2013;57(3):609–e6181. - PubMed
-
- McCabe JJ, Camps-Renom P, Giannotti N, et al. Carotid plaque inflammation imaged by PET and prediction of recurrent stroke at 5 years. Neurology. 2021;97(23):e2282–91. - PubMed
-
- Dawson LP, Lum M, Nerleker N, et al. Coronary Atherosclerotic Plaque Regression.Journal of the American College of Cardiology, 2022;;79(1): 66–82. - PubMed
LinkOut - more resources
Full Text Sources
