

Atrial dysfunction: a contrast-free marker for HFpEF in obese diabetics-insights from comprehensive CMR and serum biomarker analyses
- PMID: 40533773
- PMCID: PMC12175437
- DOI: 10.1186/s12933-025-02808-3
Atrial dysfunction: a contrast-free marker for HFpEF in obese diabetics-insights from comprehensive CMR and serum biomarker analyses
Abstract
Background: The diagnostic criteria for HFpEF remain inconsistently defined, further confounded by comorbidities such as obesity and type 2 diabetes mellitus (T2DM), which are thought to contribute to its pathogenesis via chronic pro-inflammatory mechanisms. This study aimed to evaluate the relationship between advanced cardiac magnetic resonance (CMR) imaging and pro-fibrotic and inflammatory serum biomarkers, assessing their potential to discriminate HFpEF from associated comorbid conditions.
Methods: This was an exploratory analysis of a prospective cohort study of 35 obese/overweight participants (mean age 64 ± 8 years, 23% females), including 16 with T2DM, 13 with HFpEF (NYHA II-III) and T2DM, and 6 healthy controls. All subjects underwent comprehensive contrast-enhanced CMR at a 3 T scanner (Philips Ingenia, The Netherlands), including assessment of left ventricular and left atrial (LA) volumetry and function, myocardial perfusion reserve (MPR), and diffuse fibrosis imaging (ECV). Obtained serum biomarkers were Pentraxin-3, Galectin-3 and Interleukin-1 Receptor-Like 1 (IL1RL1). Statistical analyses included one-way ANOVA, Tukey test, Pearson's correlation, regression and receiver operating characteristic analyses, and intra-class correlation.
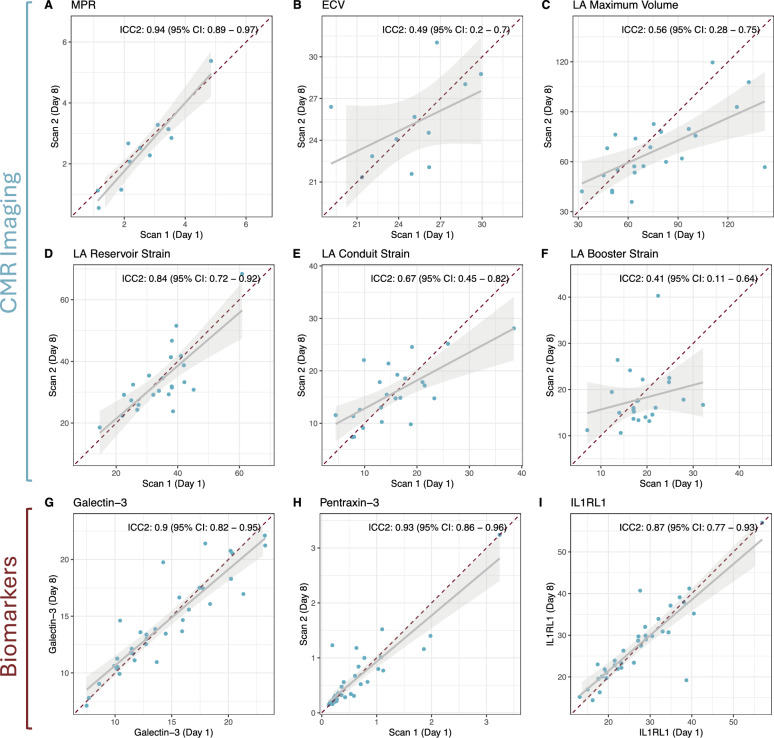
Results: In multivariable regression, impaired measures of LA structure and function emerged as the only independent discriminators of HFpEF, with LA maximum volume showing an OR of 1.13 (95% CI 1.05-1.28), reservoir strain of 0.71 (95% CI 0.44-0.89), conduit strain of 0.57 (95% CI 0.32-0.82) and booster strain of 0.70 (95% CI 0.48-0.89) per unit increase. No differences in MPR nor ECV were observed between the groups. While serum biomarkers Galectin-3 and Pentraxin-3 were significantly higher in HFpEF vs. obese controls (16.1 ng/ml ± 3.8 ng/ml vs. 10.6 ng/ml ± 3.7 ng/ml, p = 0.011, and 0.84 ng/ml ± 0.67 ng/ml vs. 0.21 ng/ml ± 0.05 ng/ml, p = 0.031, respectively), these biomarkers remained within normal limits and showed only moderate correlations with CMR metrics. Highest inter-study reproducibility was seen in MPR (ICC: 0.94), LA Reservoir Strain (ICC: 0.84) and serum biomarkers (ICC: 0.087-0.93).
Conclusion: CMR markers of diffuse fibrosis and microvascular dysfunction may not differentiate HFpEF from obese or diabetic controls. However, left atrial function assessment may evolve to be a reproducible and practical CMR marker, effectively distinguishing HFpEF independent of fibrotic remodeling.
Keywords: Biomarkers; Cardiac magnetic resonance; HFpEF; IL1RL1; Left atrial strain; Obesity; Type 2 diabetes mellitus.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interests: SK and CT report grants support by the DZHK (German Center for Cardiovascular Research), partner site Berlin, and Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—SFB1470. SK reports grants from Philips Healthcare, BioVentrix, Berlin-Chemie, MSD/Bayer, Novartis, Astra Zeneca, Siemens, and Myocardial Solutions outside of the submitted work. SK is also on the advisory board for MSD/Bayer, BioVentrix, and Myocardial Solutions. All other authors declare that they have no relationships relevant to the contents of this paper to disclose.
Figures


References
-
- Dunlay SM, Roger VL, Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2017;14(10):591–602. - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC) with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. 2021;42(36):3599–726. - PubMed
-
- Pieske B, Tschöpe C, de Boer RA, Fraser AG, Anker SD, Donal E, et al. How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the heart failure association (HFA) of the European society of cardiology (ESC). Eur Heart J. 2019;40(40):3297–317. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
