

Assessment of hypothalamic-pituitary-adrenal axis impairment and effects of hydrocortisone treatment in adults with Prader-Willi syndrome
- PMID: 40535342
- PMCID: PMC12173891
- DOI: 10.3389/fendo.2025.1517334
Assessment of hypothalamic-pituitary-adrenal axis impairment and effects of hydrocortisone treatment in adults with Prader-Willi syndrome
Abstract
Objective: The prevalence of hypothalamic-pituitary-adrenal impairment (HPAI) in adults with Prader Willi Syndrome (PWS) remains unclear despite its clinical relevance. The aim of our study was to assess the prevalence of HPA axis impairment in adults with PWS based on the results of the high dose short synacthen test (HDSST), as well as to analyze the effects of hydrocortisone (HCT) therapy in this population.
Design: Retrospective analysis.
Patients: Thirty adult patients (14 men, 16 women, aged 18-28 years) with genetically confirmed PWS. Twenty-two patients (73.3%) had been adequately treated with human recombinant growth hormone (rhGH). Due to hypogonadotropic hypogonadism, all patients received hormone replacement therapy.
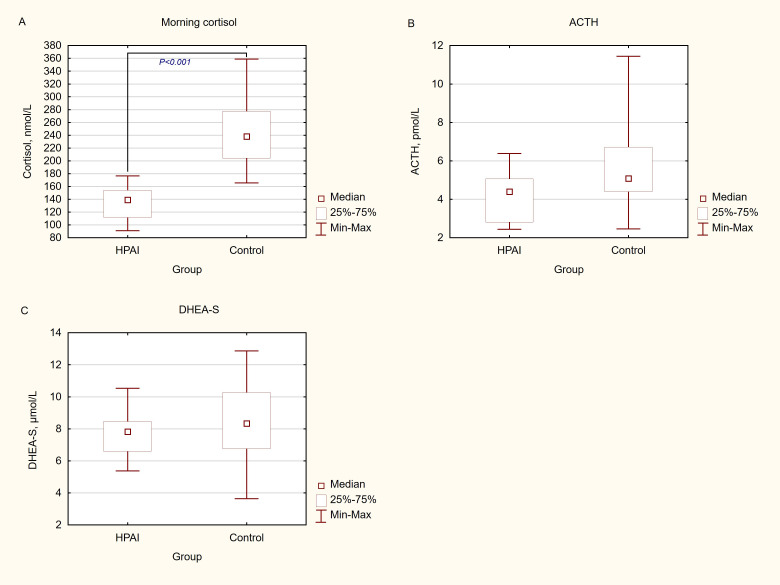
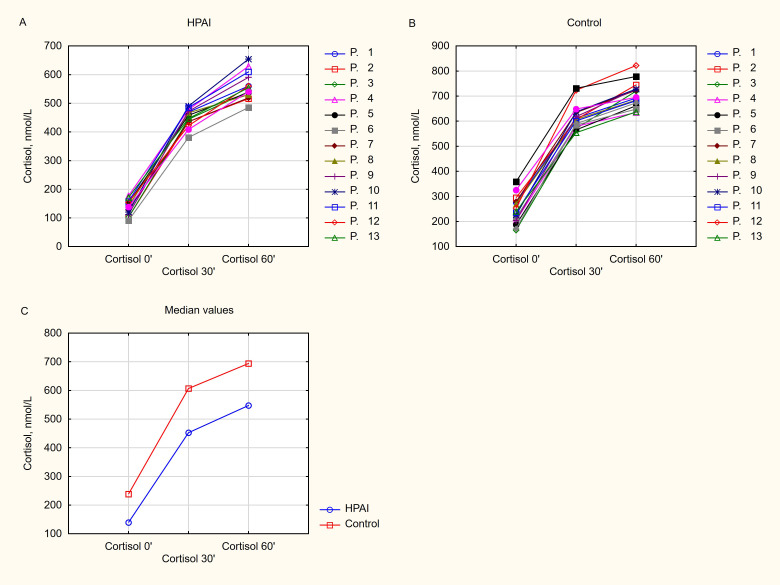
Measurements: Physical examination included measuring height, weight and body fat percentage (using the electrical bioimpedance method). Based on HDSST results, patients were divided into two groups: with HPA axis impairment (cortisol < 500 nmol/L at 30th minute), and AS (adrenal sufficiency; cortisol ≥ 500 nmol/L at the 30th minute). Clinical symptoms of adrenal insufficiency (AI), body weight and body fat percentage were evaluated at baseline, after 6 and 12 months of follow-up.
Results: Fourteen of the 30 patients (46.7%) showed a 30-min cortisol peak <500 nmol/L, and were assigned to the HPAI group. Peak cortisol levels at 30' and 60' were significantly lower in the HPAI group compared to the Control one, respectively (P<0.001) Correlation analysis revealed that basal cortisol was positively correlated with cortisol levels at both 30' and 60' of the HDSST (r = 0.872, P < 0.001 and r = 0.829, P < 0.001, respectively). Fatigue, myalgia and muscle weakness occurred more often in the HPAI group than in the Control group (90.9% vs. 20%, P= 0.01, 90.9% vs. 0%, P=0.001, respectively). All symptomatic patients with HPAI received HCT treatment (10 mg/day) in two divided doses. Fatigue, myalgiaand muscle weakness improved significantly after 12 months of HCT therapy (P<0.001). No adverse effects of HCT treatment were observed, such as weight gain, body fat percentage increase or metabolic abnormalities.
Conclusions: The results of our study suggest that the HPA axis should be routinely evaluated in adult patients with PWS. Short term, low-dose HCT treatment in symptomatic patients with HPAI is safe and can reduce symptoms of fatigue, myalgia and muscle weakness. However, the benefits and adverse effects of HCT treatment in this population require confirmation in prospective, placebo-controlled randomized clinical studies.
Keywords: Prader-Willi syndrome; adrenal insufficiency; high dose short synacthen test; hydrocortisone treatment; hypothalamic-pituitary-adrenal axis impairment; rare disease.
Copyright © 2025 Góralska, Pokrzywa, Stańczyk, Libura and Bednarczuk.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Goldstone AP, Holland AJ, Hauffa BP, Hokken-Koelega AC, Tauber M, Speakers contributors at the Second Expert Meeting of the Comprehensive Care of Patients with PWS . Recommendations for the diagnosis and management of Prader-Willi syndrome. J Clin Endocrinol Metab. (2008) 93:4183–97. doi: 10.1210/jc.2008-0649 - DOI - PubMed
-
- Góralska M, Bednarczuk T, Rosłon M, Libura M, Szalecki M, Walczak M, et al. Management of Prader-Willi Syndrome (PWS) in adults — what an endocrinologist needs to know. Recommendations Polish Soc Endocrinol Polish Soc Paediatric Endocrinol Diabetology. Endokrynologia Polska. (2018) 69:345–64. doi: 10.5603/EP.2018.0047 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials