

Diagnostic value of fasting hypopharyngeal salivary pepsin concentration test for laryngopharyngeal reflux disease
- PMID: 40535736
- PMCID: PMC12172123
- DOI: 10.1002/wjo2.200
Diagnostic value of fasting hypopharyngeal salivary pepsin concentration test for laryngopharyngeal reflux disease
Abstract
Objective: To investigate the diagnostic value of the fasting hypopharyngeal salivary pepsin concentration test for laryngopharyngeal reflux disease (LPRD).
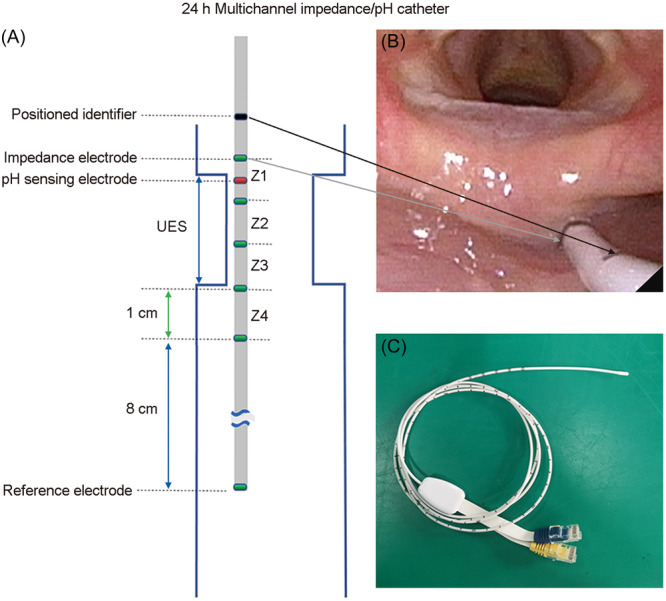
Methods: Volunteers were grouped by reflux symptom index scale, reflux finding score scale, and 24-h hypopharyngeal-esophageal multichannel intraluminal impedance with pH monitoring results. The study comprised 56, 27, and 20 individuals in the LPRD, asymptomatic laryngopharyngeal reflux (LPR), and asymptomatic non-LPR groups, respectively. All underwent a fasting hypopharyngeal saliva pepsin testing via enzyme-linked immunosorbent assay. Statistical analysis determined the optimal diagnostic cutoff value, sensitivity, and specificity of hypopharyngeal salivary pepsin for LPRD. Correlation analysis was performed with reflux scale scores and LPR parameters.
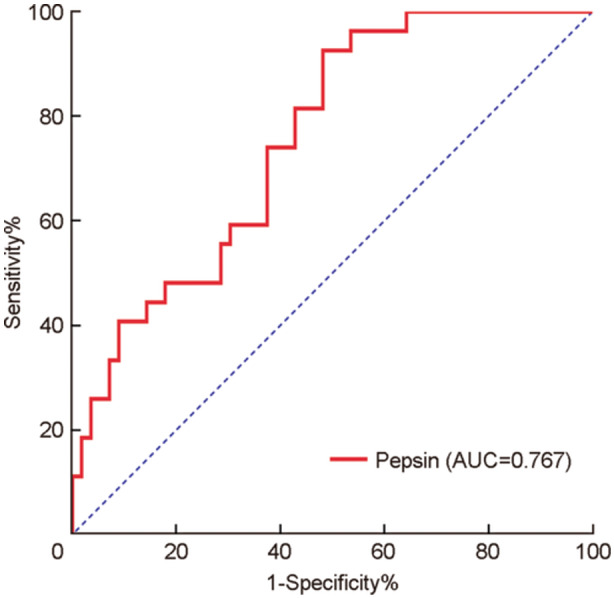
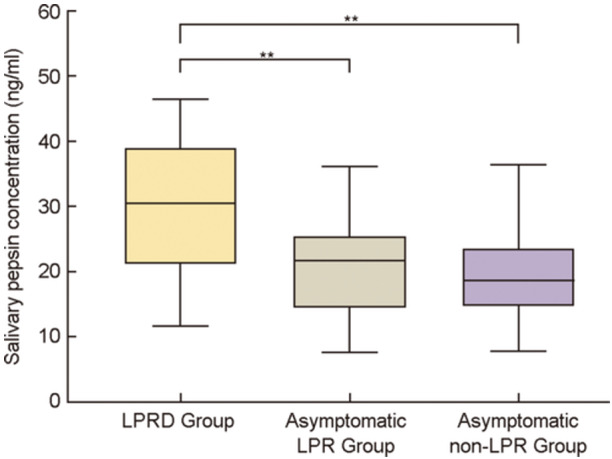
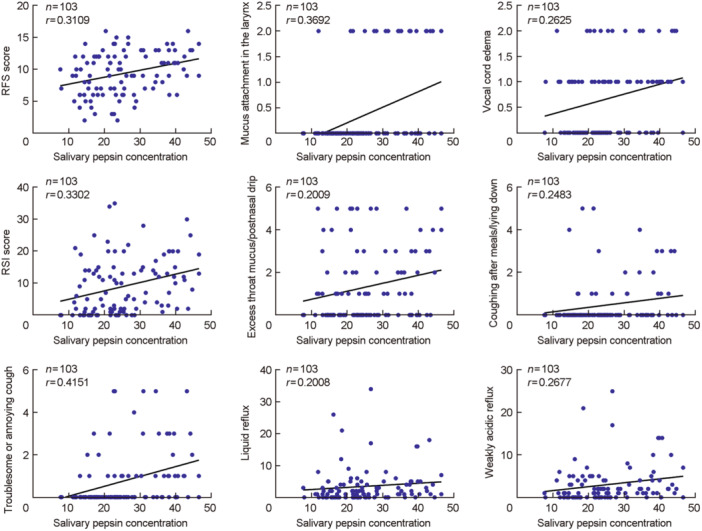
Results: Fasting hypopharyngeal salivary pepsin concentration in the LPRD group was significantly higher than in the asymptomatic control group (Z = -4.724, p < 0.05). The area under the receiver operating characteristic curve (AUC) analysis identified an optimal cutoff value of 29.62 ng/mL for salivary pepsin concentration (AUC, 0.767; sensitivity, 51.8%; and specificity, 93.6%). There was no statistically significant difference in salivary pepsin concentration between the asymptomatic LPR and non-LPR groups. The concentration was higher in the LPRD group than in the asymptomatic LPR and non-LPR groups (p < 0.05). Fasting hypopharyngeal salivary pepsin concentration exhibited a weakly positive correlation with vocal cord edema, intralaryngeal mucus adherence, excess throat mucus or postnasal drip, coughing during meals/lying down, troublesome or annoying cough, and liquid and weakly acidic reflux episodes.
Conclusions: The fasting hypopharyngeal salivary pepsin concentration test is a highly specific, simple, and noninvasive method with significant clinical diagnostic value for LPRD.
Keywords: diagnosis; fasting; hypopharynx; laryngopharyngeal reflux disease; saliva pepsin.
© 2024 The Author(s). World Journal of Otorhinolaryngology ‐ Head and Neck Surgery published by John Wiley & Sons Ltd on behalf of Chinese Medical Association.
Conflict of interest statement
Professor Ting Chen is a member of the World Journal of Otorhinolaryngology‐Head & Neck Surgery (WJOHNS) editorial board and is not involved in the peer review process of this article. Other authors declare no conflict of interest.
Figures
Similar articles
-
Diagnostic utility of salivary pepsin in laryngopharyngeal reflux: a systematic review and meta-analysis.Braz J Otorhinolaryngol. 2023 Mar-Apr;89(2):339-347. doi: 10.1016/j.bjorl.2022.10.050. Epub 2022 Oct 29. Braz J Otorhinolaryngol. 2023. PMID: 36347787 Free PMC article.
-
Predictive Value of Digestive Enzymes in Patients With Reflux-Induced Chronic Cough.Otolaryngol Head Neck Surg. 2025 Aug;173(2):453-460. doi: 10.1002/ohn.1283. Epub 2025 May 2. Otolaryngol Head Neck Surg. 2025. PMID: 40317959
-
Acid Assault: Unmasking the Toll of Laryngopharyngeal Reflux Disease on Vocal Health - A Literature Review.Indian J Otolaryngol Head Neck Surg. 2025 Feb;77(2):1160-1164. doi: 10.1007/s12070-024-05279-2. Epub 2024 Dec 24. Indian J Otolaryngol Head Neck Surg. 2025. PMID: 40070741
-
Increased Sensitivity of Cough Reflex is Not the Mechanism of Cough Attributed to Laryngopharyngeal Reflux.J Voice. 2025 Jul;39(4):903-910. doi: 10.1016/j.jvoice.2023.02.019. Epub 2023 Apr 23. J Voice. 2025. PMID: 37095027
-
Is Pepsin a Reliable Marker of Laryngopharyngeal Reflux? A Systematic Review.Otolaryngol Head Neck Surg. 2017 Sep;157(3):385-391. doi: 10.1177/0194599817709430. Epub 2017 Jun 6. Otolaryngol Head Neck Surg. 2017. PMID: 28585488
References
-
- Subspecialty Group of Laryngopharyngology, Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery . Experts consensus on diagnosis and treatment of laryngopharyngeal reflux disease (2022). Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022;57(10):1149‐1172. - PubMed
-
- Xiao S, Li J, Zheng H, et al. An epidemiological survey of laryngopharyngeal reflux disease at the otorhinolaryngology‐head and neck surgery clinics in China. Eur Arch Otrhinolaryngol. 2020;277:2829‐2838. - PubMed
-
- Francis DO, Rymer JA, Slaughter JC, et al. High economic burden of caring for patients with suspected extraesophageal reflux. Am J Gastroenterol. 2013;108:905‐911. - PubMed
-
- Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux symptom index (RSI). J Voice. 2002;16:274‐277. - PubMed
-
- Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope. 2001;111:1313‐1317. - PubMed
LinkOut - more resources
Full Text Sources