

Comparative Analysis of Clinical Outcomes and Financial Aspects of Phototherapies and Immunotherapy for Cancer
- PMID: 40536322
- PMCID: PMC12376634
- DOI: 10.1002/advs.202417657
Comparative Analysis of Clinical Outcomes and Financial Aspects of Phototherapies and Immunotherapy for Cancer
Abstract
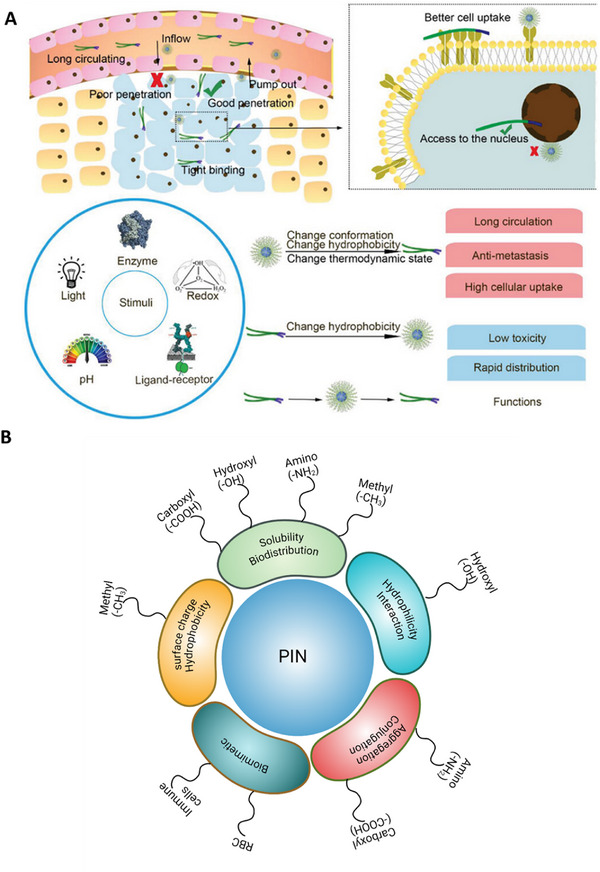
Photo-responsive/activable nanomedicine-driven therapies have emerged as a transformative approach to effectively target and eliminate tumors across different types of solid cancers. When synergistically combined with immunomodulators, these therapies significantly enhance anti-cancer efficacy. This comprehensive review examines the current advancements in photo-responsive/activable immunomodulator-loaded nanomedicines (PINs), providing a detailed analysis of their preclinical development, clinical translation, and associated research funding. The diverse PINs are systematically categorized, innovative design strategies are explored, and the underlying photo-responsive/activable and immunomodulatory mechanisms are elucidated. By integrating clinical advancements with technical innovations and financial perspectives, this review bridges the translational gap, underscoring the immense potential of PINs to revolutionize cancer therapy. This comprehensive resource is indispensable for researchers striving to bring phototherapies to clinical fruition in the battle against cancer.
Keywords: clinical trials; immunotherapy; photodynamic therapy; photoimmunotherapy; photothermal therapy.
© 2025 The Author(s). Advanced Science published by Wiley‐VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







Similar articles
-
Innovative approaches for cancer treatment: graphene quantum dots for photodynamic and photothermal therapies.J Mater Chem B. 2024 May 8;12(18):4307-4334. doi: 10.1039/d4tb00255e. J Mater Chem B. 2024. PMID: 38595268 Review.
-
Driving Best Practices Throughout the Treatment Journey for Patients with NSCLC with Actionable Alterations: A Podcast Discussion.Adv Ther. 2025 Aug;42(8):3591-3605. doi: 10.1007/s12325-025-03195-7. Epub 2025 May 22. Adv Ther. 2025. PMID: 40402375 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Overcoming resistant cancerous tumors through combined photodynamic and immunotherapy (photoimmunotherapy).Front Immunol. 2025 Jul 17;16:1633953. doi: 10.3389/fimmu.2025.1633953. eCollection 2025. Front Immunol. 2025. PMID: 40746528 Free PMC article. Review.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
References
-
- a) Vats M., Mishra S. K., Baghini M. S., Chauhan D. S., Srivastava R., De A., Int. J. Mol. Sci. 18, 924; - PMC - PubMed
- b) Chauhan D. S., Kumawat M. K., Prasad R., Reddy P. K., Dhanka M., Mishra S. K., Bahadur R., Neekhra S., De A., Srivastava R., Colloids Surf., B 2018, 172, 430; - PubMed
- c) Chauhan D. S., Bukhari A. B., Ravichandran G., Gupta R., George L., Poojari R., Ingle A., Rengan A. K., Shanavas A., Srivastava R., De A., Sci. Rep. 2018, 8, 16673; - PMC - PubMed
- d) Chauhan D. S., Arunkumar P., Prasad R., Mishra S. K., BP K. R., De A., Srivastava R., Mater. Sci. Eng., C 2018, 90, 539; - PubMed
- e) Fan F., Hou Y., Zhang Y., Zeng Y., Zhang Y., Zhang S., Meng X., Wang X., Front. Oncol. 2022, 12, 987491; - PMC - PubMed
- f) Qin L., Cao J., Shao K., Tong F., Yang Z., Lei T., Wang Y., Hu C., Umeshappa C. S., Gao H., Peppas N. A., Sci. Adv. 2020, 6, 3116; - PMC - PubMed
- g) Hu C., Lei T., Wang Y., Cao J., Yang X., Qin L., Liu R., Zhou Y., Tong F., Umeshappa C. S., Gao H., Biomaterials 2020, 255, 120159. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous