

Giant-cell rich osteosarcoma: A report of 3 cases depicting a diagnostic challenge requiring serious attention
- PMID: 40536367
- PMCID: PMC12147397
- DOI: 10.5152/j.aott.2025.24076
Giant-cell rich osteosarcoma: A report of 3 cases depicting a diagnostic challenge requiring serious attention
Abstract
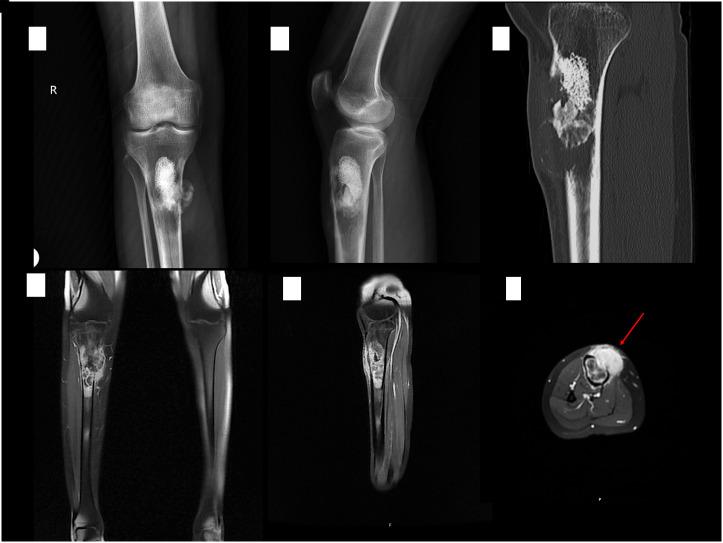
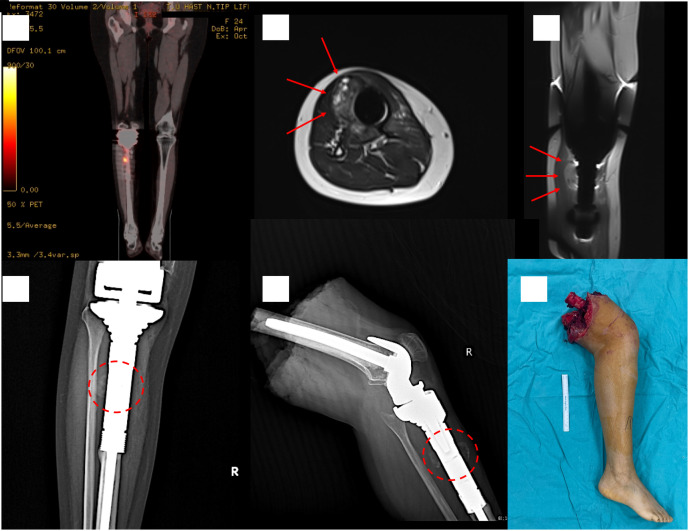
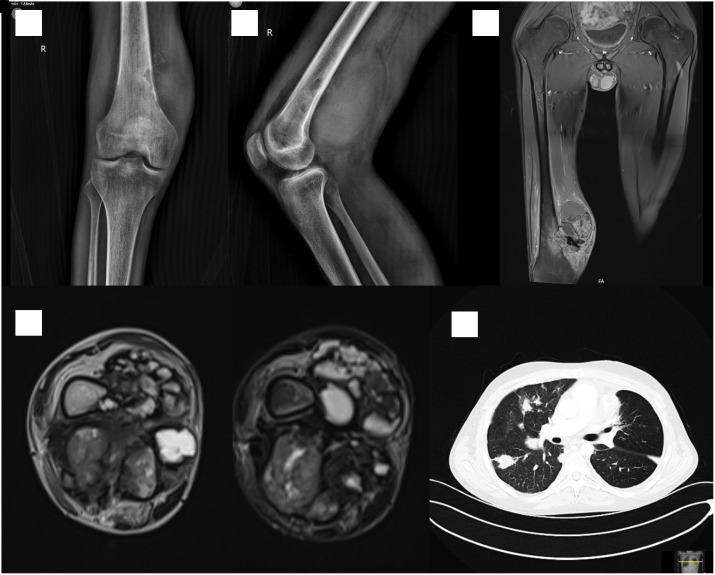
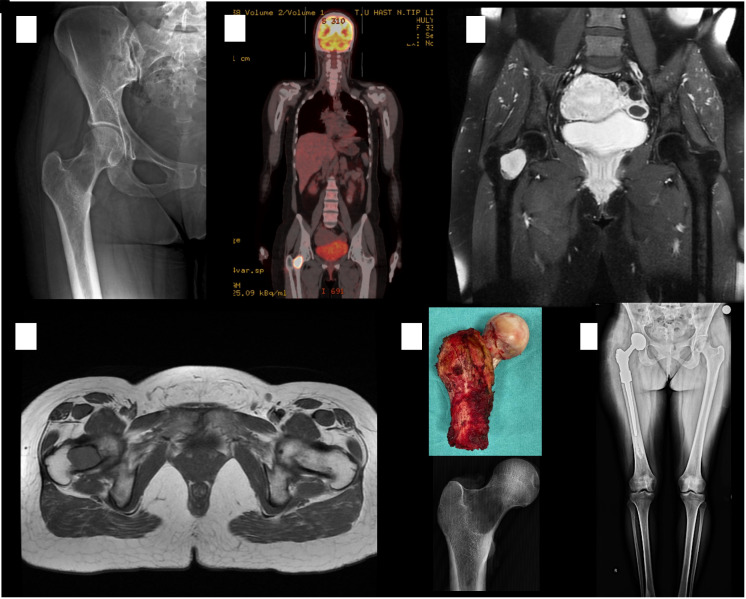
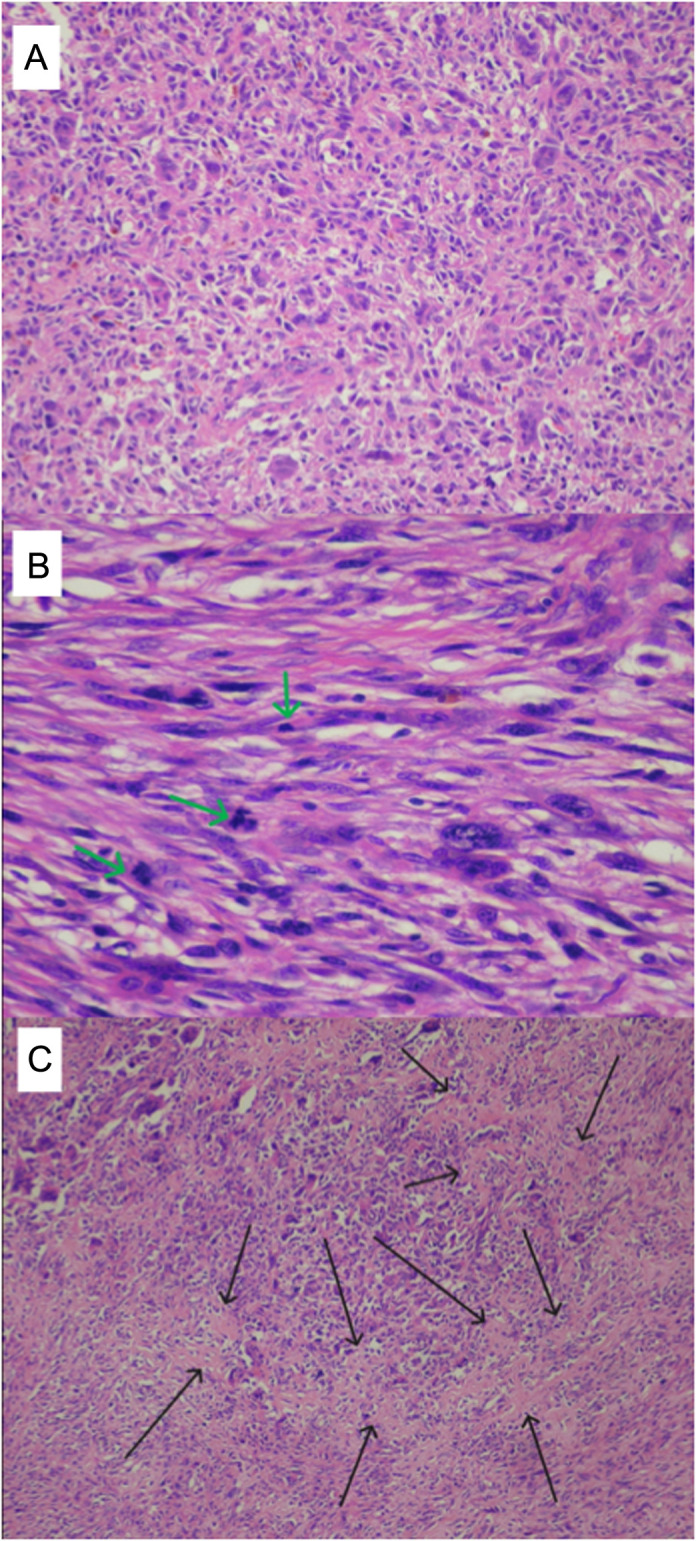
Giant cell-rich osteosarcoma (GCRO) is a rare variant of osteosarcoma with unusual radiological and histopathological features that make its diagnosis challenging. The most critical and unusual feature of GCRO is that it has a purely osteolytic appearance. Therefore, GCRO cases are frequently subject to delayed diagnosis or incorrect treatment owing to misdiagnosis. This negatively affects the prognosis of these patients. In this study, 3 young adult cases are presented. The first case describes a young female patient who underwent repeated curettages due to a misdiagnosis of a giant-cell bone tumor, and the second case describes a delay in diagnosis in a young male patient who was misdiagnosed with an aneurysmal bone cyst. The final case report describes a young woman who was diagnosed early, treated promptly, and had a good prognosis. One of the poor prognosis cases in this report was treated with amputation, and the other was alive with multiple metastases. Misdiagnosis or delayed diagnosis leads to a poor prognosis in such cases. To make a diagnosis, it is necessary to have knowledge and to be suspicious of the radiological features of this rare variant. Giant cell-rich osteosarcoma should be among the differential diagnosis options when dealing with pure metaphysiodiaphyseal osteolytic bone lesions in young adults. To avoid misdiagnosis or delay, it is necessary to have knowledge and to be suspicious of this rare variant. Level of Evidence: Level IV, Therapeutic study.
Conflict of interest statement
Figures
References
-
- Campanacci M. In: Campanacci M, ed. Bone and Soft Tissue Tumors: Clinical Features, Imaging, Pathology and Treatment. Springer; Vienna, Vienna; 1999:1 70. ( 10.1007/978-3-7091-3846-5_1) - DOI
-
- Campanacci M. High grade osteosarcomas. In: Campanacci M, ed. Bone and Soft Tissue Tumors: Clinical Features, Imaging, Pathology and Treatment. Springer; Vienna, Vienna; 1999:463 515. ( 10.1007/978-3-7091-3846-5_28) - DOI
-
- Picci P. Classic osteosarcoma. In: Picci P, Manfrini M, Fabbri N, Gambarotti M, Vanel D, eds. Atlas of Musculoskeletal Tumors and Tumorlike Lesions: the Rizzoli Case Archive. Springer International Publishing, Cham; 2014:147 152. ( 10.1007/978-3-319-01748-8_34) - DOI
-
- Hong SJ, Kim KA, Yong HS, et al. Giant cell-rich osteosarcoma of bone. Eur J Rad Extra. 2005;53(2):87 90. ( 10.1016/j.ejrex.2004.12.001) - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
