

ECG Abnormalities and Biomarkers Enable Rapid Risk Stratification in Normotensive Patients With Acute Pulmonary Embolism
- PMID: 40536791
- PMCID: PMC12178209
- DOI: 10.1111/crj.70060
ECG Abnormalities and Biomarkers Enable Rapid Risk Stratification in Normotensive Patients With Acute Pulmonary Embolism
Abstract
Background: The patients with suspected pulmonary embolism (PE) were usually screened using electrocardiogram (ECG) and blood panel of D-dimer, troponin, and blood gas analysis in the emergency.
Objectives: This study aimed to explore a rapid risk model to predict in-hospital adverse events for normotensive PE patients.
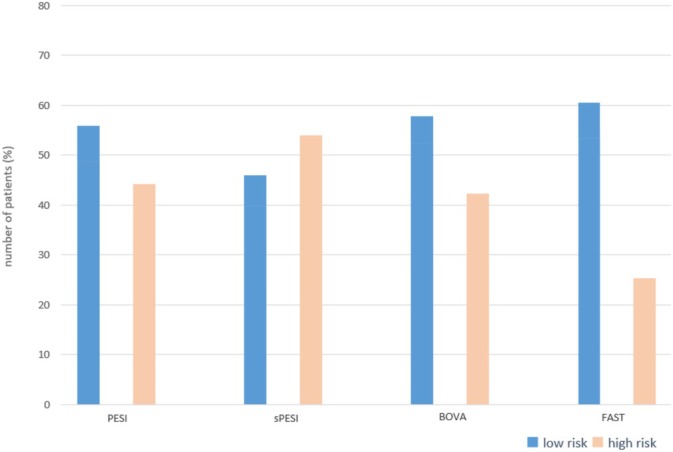
Methods: Patients with acute PE having normal blood pressure on appearance were retrospectively enrolled at China-Japan Friendship Hospital from January 2017 to February 2020. The in-hospital adverse events were defined as death and clinical deterioration during hospitalization. The risk model for in-hospital adverse events was generated by multivariate regression analysis. The discrimination ability of the model was compared with PESI, Bova, and FAST risk score, and evaluated by the receiver operating characteristic curve (ROC), net reclassification improvement (NRI), and integrated discrimination improvement index (IDI).
Results: Of the 213 patients, 35 (16.4%) experienced in-hospital adverse events,y including 15 deaths. The average age was 69 ± 19 years, and 118 (44.6%) were females. Multiple logistic regression analysis showed that independent risk factors associated with in-hospital adverse events were low QRS voltage in ECG (OR: 5.321; 95% CI: 1.608-7.310), positive age-adjusted D-dimer (OR: 2.061; 95% CI: 0.622-6.836), positive troponin (OR: 3.504; 95% CI: 1.744-8.259), and PaO2/FiO2 < 300 (OR: 3.268; 95% CI: 0.978-5.260). The ROC analysis showed that the AUC of the new model (0.847, 95% CI: 0.786-0.901) was better than the PESI score (0.628, 95% CI: 0.509-0.769), the Bova score (0.701, 95% CI: 0.594-0.808), and the FAST score (0.775 95% CI: 0.690-0.859).
Conclusion: ECG abnormalities and biomarkers on admission may provide a rapid and effective approach to identify patients with poor prognoses during hospitalization.
Keywords: acute pulmonary embolism; in‐hospital adverse events; low to moderate risk; prognosis.
© 2025 The Author(s). The Clinical Respiratory Journal published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
The Prognostic Role of Hematological Markers in Acute Pulmonary Embolism: Enhancing Risk Stratification.Medicina (Kaunas). 2025 Jun 17;61(6):1095. doi: 10.3390/medicina61061095. Medicina (Kaunas). 2025. PMID: 40572783 Free PMC article.
-
Predicting Deterioration in Patients With Normotensive Acute Pulmonary Embolism Using Clinical-Imaging Features: A Multicenter Prospective Cohort Study.J Am Heart Assoc. 2025 Jul;14(13):e038984. doi: 10.1161/JAHA.124.038984. Epub 2025 Jun 27. J Am Heart Assoc. 2025. PMID: 40576035
-
Venous lactate as a tool for the Risk-Stratification of patients with acute pulmonary embolism: A retrospective cohort study.Clin Biochem. 2025 Aug;138:110942. doi: 10.1016/j.clinbiochem.2025.110942. Epub 2025 May 8. Clin Biochem. 2025. PMID: 40348120
-
Troponin-based risk stratification of patients with acute nonmassive pulmonary embolism: systematic review and metaanalysis.Chest. 2009 Oct;136(4):974-982. doi: 10.1378/chest.09-0608. Epub 2009 May 22. Chest. 2009. PMID: 19465511
-
Prognostic value of troponins in acute nonmassive pulmonary embolism: A meta-analysis.Heart Lung. 2015 Jul-Aug;44(4):327-34. doi: 10.1016/j.hrtlng.2015.03.007. Epub 2015 May 11. Heart Lung. 2015. PMID: 25976228
References
-
- Becattini C., Agnelli G., Lankeit M., et al., “Acute Pulmonary Embolism: Mortality Prediction by the 2014 European Society of Cardiology Risk Stratification Model,” European Respiratory Journal 48, no. 3 (2016): 780–786. - PubMed
-
- Donzé J., Le Gal G., Fine M. J., et al., “Prospective Validation of the Pulmonary Embolism Severity Index. A Clinical Prognostic Model for Pulmonary Embolism,” Thrombosis and Haemostasis 100, no. 5 (2008): 943–948. - PubMed
-
- Righini M., Roy P. M., Meyer G., Verschuren F., Aujesky D., and Le Gal G., “The Simplified Pulmonary Embolism Severity Index (PESI): Validation of a Clinical Prognostic Model for Pulmonary Embolism,” Journal of Thrombosis and Haemostasis 9, no. 10 (2011): 2115–2117. - PubMed
-
- Hobohm L., Hellenkamp K., Hasenfuß G., Münzel T., Konstantinides S., and Lankeit M., “Comparison of Risk Assessment Strategies for Not‐High‐Risk Pulmonary Embolism,” European Respiratory Journal 47, no. 4 (2016): 1170–1178. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
