

Blood immunophenotyping identifies distinct kidney histopathology and outcomes in patients with lupus nephritis
- PMID: 40536813
- PMCID: PMC12352894
- DOI: 10.1172/JCI181034
Blood immunophenotyping identifies distinct kidney histopathology and outcomes in patients with lupus nephritis
Abstract
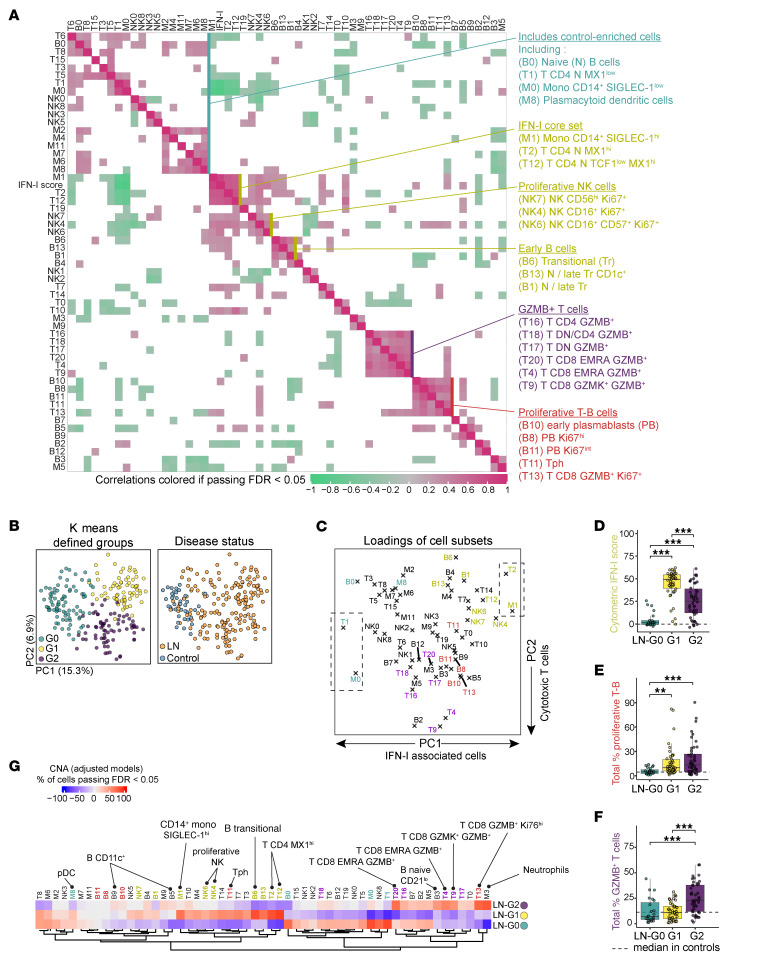
Lupus nephritis (LN) is a frequent manifestation of systemic lupus erythematosus, and fewer than half of patients achieve complete renal response with standard immunosuppressants. Identifying noninvasive, blood-based immune alterations associated with renal injury could aid therapeutic decisions. Here, we used mass cytometry immunophenotyping of peripheral blood mononuclear cells in 145 patients with biopsy-proven LN and 40 healthy controls to evaluate the heterogeneity of immune activation and identify correlates of renal parameters. Unbiased analysis identified 3 immunologically distinct groups of patients that were associated with different patterns of histopathology, renal cell infiltrates, urine proteomic profiles, and treatment response at 1 year. Patients with enriched circulating granzyme B+ T cells showed more active disease and increased numbers of activated CD8+ T cells in the kidney, yet they had the highest likelihood of treatment response. A second group characterized by a high type I interferon signature had a lower likelihood of response to therapy, while a third group appeared immunologically inactive but with chronic renal injuries. The major immunologic axes of variation could be distilled down to 5 simple cytometric parameters that recapitulate several clinical associations, highlighting the potential for blood immunoprofiling to translate to clinically useful noninvasive metrics to assess immune-mediated disease in LN.
Keywords: Autoimmunity; Biomarkers; Immunology; Lupus.
Figures





Update of
-
Blood immunophenotyping identifies distinct kidney histopathology and outcomes in patients with lupus nephritis.bioRxiv [Preprint]. 2024 Mar 9:2024.01.14.575609. doi: 10.1101/2024.01.14.575609. bioRxiv. 2024. Update in: J Clin Invest. 2025 Jun 19;135(16):e181034. doi: 10.1172/JCI181034. PMID: 38293222 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
- UH2 AR067685/AR/NIAMS NIH HHS/United States
- UM2 AR067678/AR/NIAMS NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- UH2 AR067681/AR/NIAMS NIH HHS/United States
- UH2 AR067688/AR/NIAMS NIH HHS/United States
- UH2 AR067689/AR/NIAMS NIH HHS/United States
- UH2 AR067690/AR/NIAMS NIH HHS/United States
- UH2 AR067677/AR/NIAMS NIH HHS/United States
- UH2 AR067694/AR/NIAMS NIH HHS/United States
- UH2 AR067679/AR/NIAMS NIH HHS/United States
- UH2 AR067676/AR/NIAMS NIH HHS/United States
- UH2 AR067691/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
