

Risk of Cardiovascular Disease in Cancer Survivors after Systemic Treatment: A Population-Based Cohort Study
- PMID: 40537185
- PMCID: PMC12228137
- DOI: 10.1016/j.jaccao.2025.03.008
Risk of Cardiovascular Disease in Cancer Survivors after Systemic Treatment: A Population-Based Cohort Study
Abstract
Background: Patients face an increased risk of cardiovascular disease shortly after a cancer diagnosis, but evidence on long-term risk among cancer survivors remains limited.
Objectives: In this study the authors sought to estimate the risk of cardiovascular disease in cancer survivors previously treated with systemic cancer therapy.
Methods: Using Danish population-based registries, we identified individuals who had received systemic cancer treatment and were free of both cancer and treatment 3 years after diagnosis (index date). For each cancer survivor, 5 cancer-free individuals from the general population were randomly selected, matched by birth year, sex, and calendar year. Participants were followed from the index date for up to 5 years. HRs were estimated using Cox regression, adjusted for potential confounders.
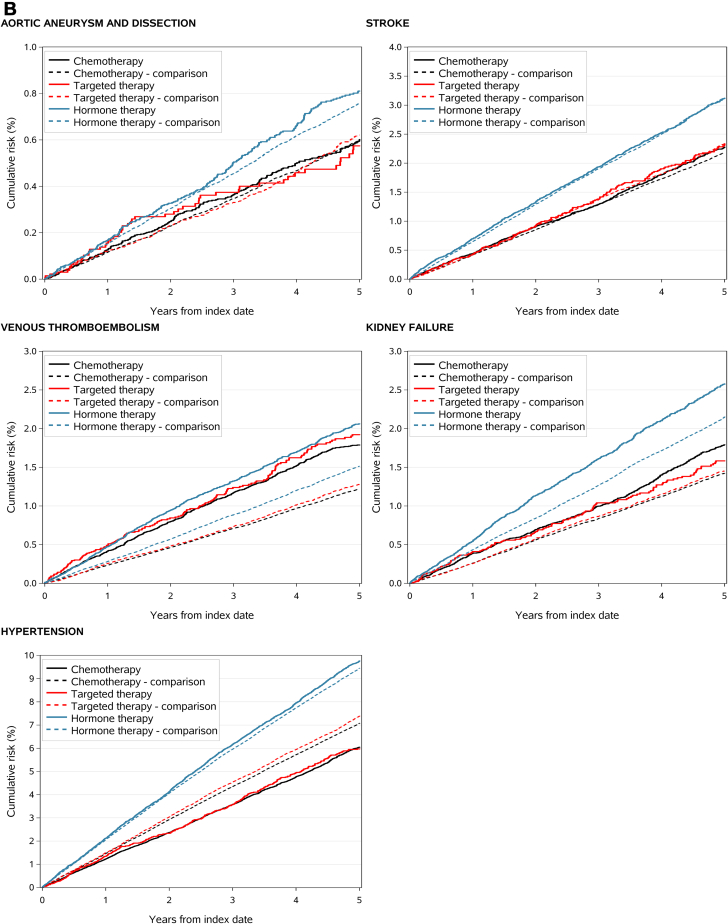
Results: Compared with 457,035 matched individuals, the 91,407 cancer survivors had an increased risk of heart failure or cardiomyopathy (HR: 1.08; 95% CI: 1.02-1.15), venous thromboembolism (HR: 1.50; 95% CI: 1.41-1.61), pericarditis, endocarditis, or myocarditis (HR: 1.30; 95% CI: 1.11-1.52), and kidney failure (HR: 1.17; 95% CI: 1.10-1.25), but not of ischemic heart disease, stroke, or atrial fibrillation. Estimates varied substantially by cancer type and treatment agent. For example, venous thromboembolism risk was consistently increased across nearly all cancer types, whereas hypertension risk was elevated for none. Ischemic heart disease risk was increased only among lung cancer survivors. Stroke was associated with platinum compounds but not with other systemic treatments.
Conclusions: Several cardiovascular disease risks were elevated among cancer survivors, with substantial variation by cancer type and treatment.
Keywords: acute coronary syndrome; arrhythmia; cancer; cancer survivorship; cohort study; epidemiology; kidney failure; myocardial infarction; neoplasm; stroke; venous thromboembolism.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by a research grant from the Karen Elise Jensen Foundation. Dr van Es is supported by an Amsterdam Cardiovascular Sciences MD/Postdoc grant. Dr Bhaskaran is supported by a Welcome Senior Research Fellowship (220283/Z/20/Z). The Department of Clinical Epidemiology at Aarhus University receives funding for other studies from companies in the form of research grants to (and administered by) Aarhus University. None of these studies has any relation to the present study. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures











References
LinkOut - more resources
Full Text Sources
