

Ferroptosis as a potential molecular mechanism of bipolar disorder
- PMID: 40537482
- PMCID: PMC12179299
- DOI: 10.1038/s41398-025-03429-w
Ferroptosis as a potential molecular mechanism of bipolar disorder
Abstract
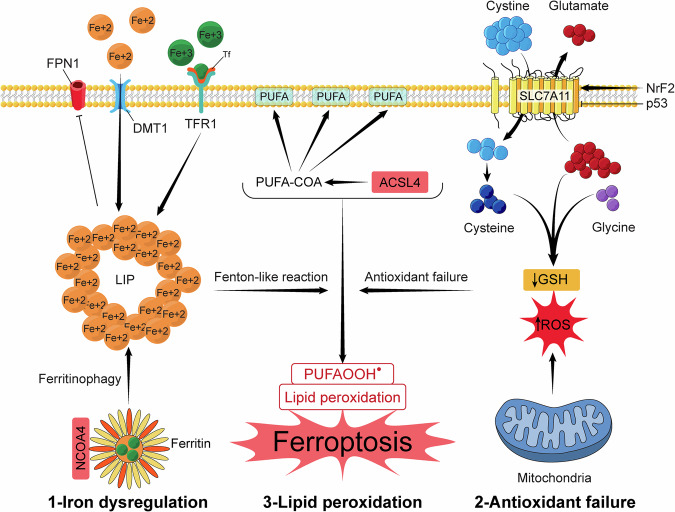
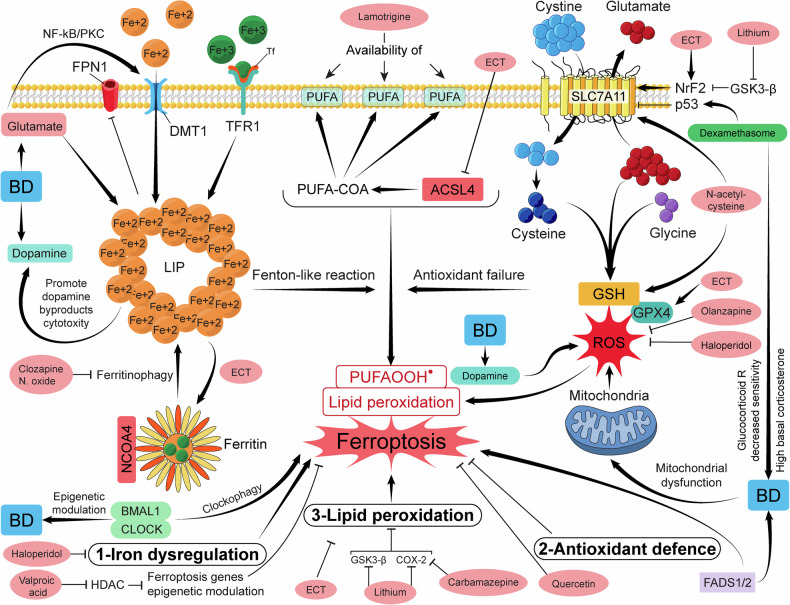
The unclear pathogenesis of bipolar disorder (BD) poses a challenge, especially with the striking rates of comorbid medical and psychiatric disorders, treatment resistance, and premature mortality in the absence of a specific diagnostic marker. We put forward the hypothesis of ferroptosis, a recently identified iron-dependent cell death, as a potential underlying mechanism of BD. We aimed to portray the possibility of ferroptosis involvement in BD pathogenesis as a doorway to encourage both animal and clinical studies on the topic. Ferroptosis is associated with multiple psychiatric disorders, including major depressive disorder, stress-induced anxiety, post-traumatic stress disorder, autism spectrum disorder, and alcohol use disorder. In addition, ferroptosis-related genes have been identified in schizophrenia, which shares genetic liabilities with BD. One of the top five most significant genes in BD in a recent genome-wide association study, FADS 2, is involved in ferroptosis. The three hallmarks of ferroptosis intersect with the pathogenesis of BD, including iron dysregulation, lipid peroxidation, and the failure of antioxidant systems. Other pieces of BD pathogenesis, including inflammation, mitochondrial dysfunction, calcium dysregulation, neurotransmission disturbance, and affection of synaptic plasticity and myelination, are either a preface or an aftermath of iron dysregulation. Additionally, circadian rhythm abnormalities and hypothalamic-pituitary-adrenal axis disturbances in BD could be another point where ferroptosis and BD intersect. Moreover, some BD treatments, such as lithium, haloperidol, olanzapine, clozapine, valproic acid, and electroconvulsive therapy, show anti-ferroptosis action in other contexts. These observations present a strong case for ferroptosis as a potential underlying mechanism of BD. Therefore, we call for studies that address iron accumulation in the brain in BD patients, postmortem tissues, and BD animal models. We call for genetic studies to look for the genetic signature of ferroptosis in BD patients. In addition, we call for studies on different BD models to assess the expression of ferroptosis markers. Our hypothesis has substantial implications if validated, including the use of ferroptosis-related genes and ferroptosis markers as a prognostic marker for BD and a potential therapeutic target based on ferroptosis inhibitors.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures

References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. American Psychiatric Publishing; 2013. pp. 591–643.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
