

Pelvic nerve endometriosis: MRI features and key findings for surgical decision
- PMID: 40537672
- PMCID: PMC12179019
- DOI: 10.1186/s13244-025-02005-6
Pelvic nerve endometriosis: MRI features and key findings for surgical decision
Abstract
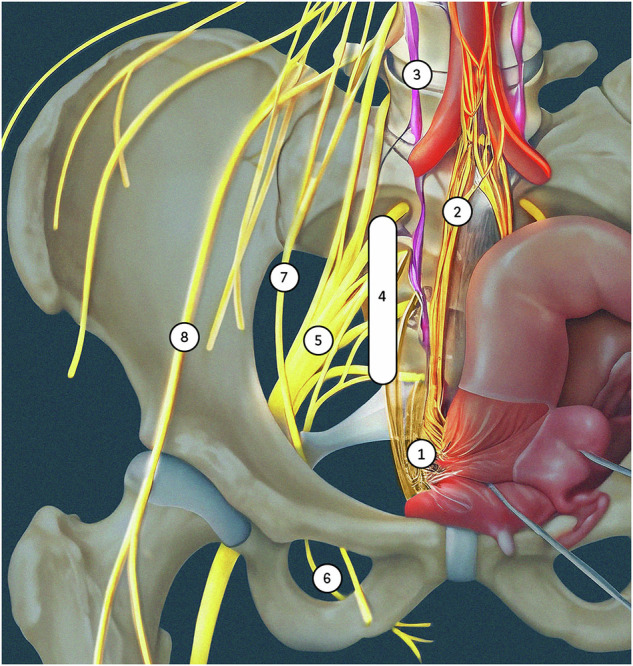
Endometriosis is a prevalent gynecological disorder in women of reproductive age. It is the leading cause of chronic pelvic pain. While the mechanisms underlying this pain remain elusive, rare cases of pelvic nerve involvement can result in severe, debilitating symptoms, adding complexity to the clinical landscape. Nerve involvement typically results from the direct extension of deep infiltrating endometriosis, though it may also occur in isolation. The nerves most commonly affected include the inferior hypogastric and lumbosacral plexuses, as well as the sciatic, pudendal, obturator, and femoral nerves. Early and accurate diagnosis is essential for the effective management of the pain and the prevention of irreversible nerve damage. Given the limitations of transvaginal ultrasonography in visualizing the lateral compartment, MRI is considered the gold standard for detecting and evaluating pelvic nerve involvement. Through the use of optimized protocols to enhance the visualization of nerves and their anatomical landmarks, radiologists play a key role in the identification of endometriotic lesions. A comprehensive and structured radiology report is essential for surgical planning, as nerve involvement often requires precise interventions to alleviate symptoms and restore quality of life. CRITICAL RELEVANCE STATEMENT: Accurate identification and a structured reporting of pelvic nerve endometriosis in the lateral compartment are pivotal to guide surgical decision-making and optimize patient outcomes. KEY POINTS: Pelvic nerve endometriosis is often overlooked, underestimated by clinicians, and underdiagnosed on imaging. Timely nerve involvement diagnosis prevents permanent damage in pelvic pain with neurological symptoms. Deep endometriosis in the lateral compartment may extend to the pelvic nerves. The inferior hypogastric plexus, sacral plexus, sciatic, and pudendal nerves are commonly affected. A dedicated MRI protocol with 3D T2-weighted sequence ensures accurate pelvic nerve assessment.
Keywords: Endometriosis; Magnetic resonance imaging; Pelvic pain; Pelvic plexus.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Consent for publication: Written informed consent was not required for this educational review because of its retrospective design and nature. No patients can be identified in the images or clinical information presented in this educational review. Competing interests: Pascal Rousset reported consultant fees from Ziwig and EDAP TMS France, reported receiving lecture fees from Bracco, General Electric Health care, and compensation for serving on the board from Guerbet. Isabelle Thomassin-Naggara reported receiving lecture fees from General Electric, Siemens, Canon, and GSK; lecture fees and compensation for serving on the board from Guerbet; compensation for serving on the board from Bayer; lecture fees from Incepto, ICAD, Fujifilm, and Hologic; and lecture fees and compensation for serving on the board from Bracco. François Golfier reported consultant fees from ZIWIG.
Figures
Similar articles
-
Surgical interventions for the management of chronic pelvic pain in women.Cochrane Database Syst Rev. 2021 Dec 20;12(12):CD008212. doi: 10.1002/14651858.CD008212.pub2. Cochrane Database Syst Rev. 2021. PMID: 34923620 Free PMC article.
-
Oral contraceptives for pain associated with endometriosis.Cochrane Database Syst Rev. 2018 May 22;5(5):CD001019. doi: 10.1002/14651858.CD001019.pub3. Cochrane Database Syst Rev. 2018. PMID: 29786828 Free PMC article.
-
Interventions for interpersonal communication about end of life care between health practitioners and affected people.Cochrane Database Syst Rev. 2022 Jul 8;7(7):CD013116. doi: 10.1002/14651858.CD013116.pub2. Cochrane Database Syst Rev. 2022. PMID: 35802350 Free PMC article.
-
Pre and post operative medical therapy for endometriosis surgery.Cochrane Database Syst Rev. 2004;2004(3):CD003678. doi: 10.1002/14651858.CD003678.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2020 Nov 18;11:CD003678. doi: 10.1002/14651858.CD003678.pub3. PMID: 15266496 Free PMC article. Updated.
-
The Hôtel-Dieu MRI Classification of Uterosacral Ligament Involvement in Endometriosis: A Pictorial Guide to Clinical Use.Diagnostics (Basel). 2025 Jun 13;15(12):1508. doi: 10.3390/diagnostics15121508. Diagnostics (Basel). 2025. PMID: 40564829 Free PMC article. Review.
References
-
- Bourgioti C, Preza O, Panourgias E et al (2017) MR imaging of endometriosis: spectrum of disease. Diagn Interv Imaging 98:751–767. 10.1016/j.diii.2017.05.009 - PubMed
-
- Tomassetti C, Johnson NP, Petrozza J et al (2021) An international terminology for endometriosis, 2021. J Minim Invasive Gynecol 28:1849–1859. 10.1016/j.jmig.2021.08.032 - PubMed
-
- Siquara De Sousa AC, Capek S, Amrami KK, Spinner RJ (2015) Neural involvement in endometriosis: review of anatomic distribution and mechanisms: neural involvement in endometriosis: review. Clin Anat 28:1029–1038. 10.1002/ca.22617 - PubMed
-
- Possover M, Chiantera V (2007) Isolated infiltrative endometriosis of the sciatic nerve: a report of three patients. Fertil Steril 87:417.e17–417.e19. 10.1016/j.fertnstert.2006.05.084 - PubMed
LinkOut - more resources
Full Text Sources
