

Prediction of peri-operative mortality in care of preterm children in non-cardiac surgery
- PMID: 40537757
- PMCID: PMC12180206
- DOI: 10.1186/s12871-025-03168-x
Prediction of peri-operative mortality in care of preterm children in non-cardiac surgery
Abstract
Background: The aim of this study was to develop a risk calculation model for peri-operative 30-day-mortality in preterm infants in non-cardiac surgery.
Methods: Retrospective monocentric follow-up cohort-study of 27,453 pediatric anesthesias at a German university hospital and level one perinatal center between 2008 and 2021 for non-cardiac surgeries. Inclusion criteria were age < 37 post-menstrual weeks at the time of surgery. The primary endpoint was 30-day-mortality after surgery. For statistical analysis, stepwise backwards logistic regressions were performed to identify predictors for 30-day mortality after surgery.
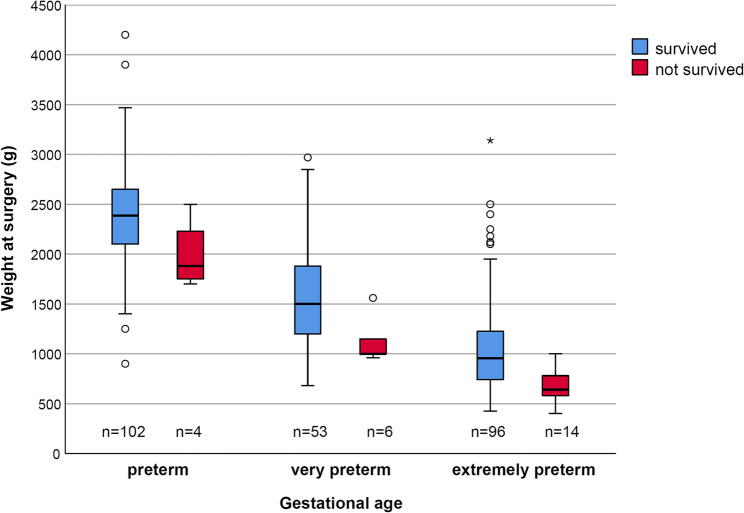
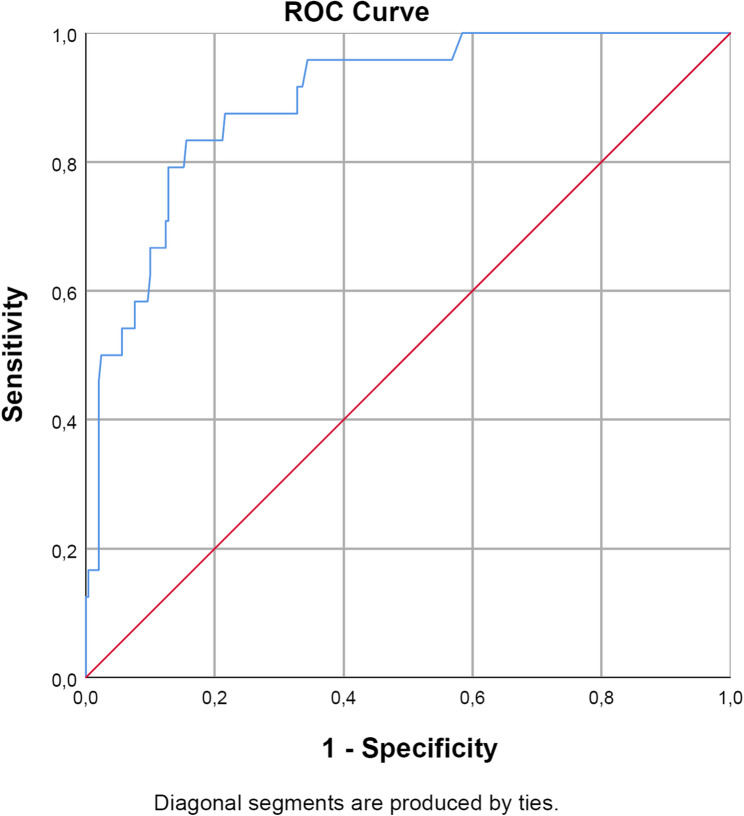
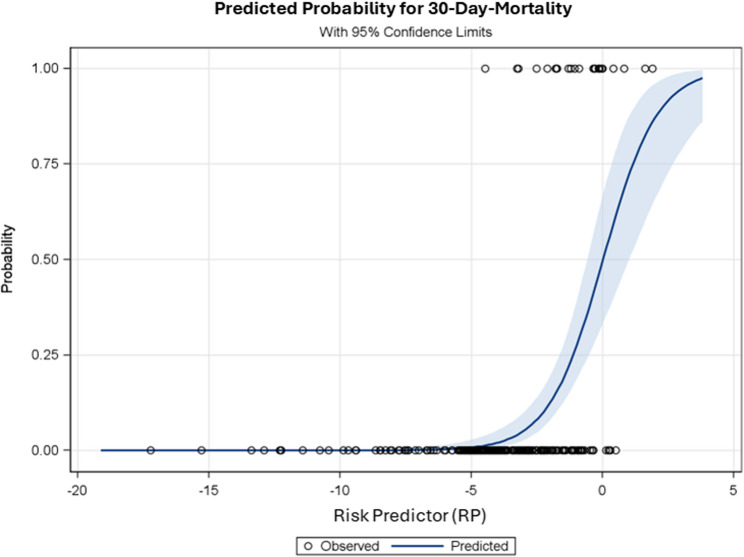
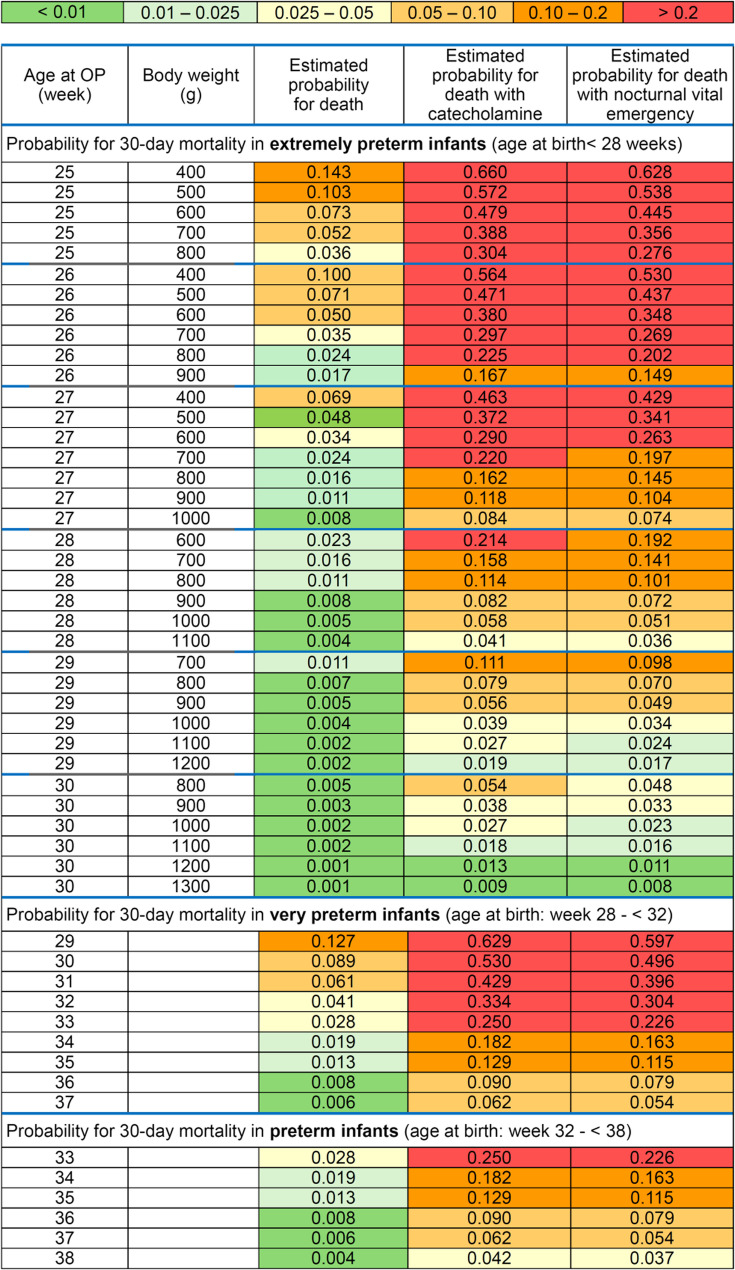
Results: Between 2007 and 2021, 278 preterm infants underwent surgery. The 30-day-mortality was 8.6% (24/278; CI95%:5.6–12.6). A preselection of potential risk factors was based primarily on prior knowledge available from the literature and the results of previously published studies. The final prediction model using a multivariable logistic regression revealed lower post-menstrual age (odds-ratio(OR): 0.67; CI95%: 0.54–0.83) and lower body weight at the time of surgery for extremely preterm infants (OR: 0.024; CI95%: 0.003–0.22), administration of dopamine or norepinephrine or epinephrine (OR: 11.6; CI95%: 3.58–37.7), and life-threatening emergencies between 10pm-7am (OR: 10.1; CI95%: 2.36–43.5) as significant independent risk factors for 30-day-mortality. The Area-Under-The-Receiver-Operating-Characteristic-Curve (0.90; CI95%: 0.85–0.96) showed a good discrimination of the final model. The investigation of the calibration curve (p = 0.99, Spiegelhalter test) and the goodness of fit test (p = 0.85, Hosmer-Lemeshow test) indicated no significant discrepancies between estimated and observed probabilities for the peri-operative 30-day mortality.
Conclusions: Peri-operative 30-day-mortality of preterm infants during non-cardiac surgery is high. The prediction model with easily ascertainable factors as described could be a valuable tool for estimating 30-day-mortality in preterm infants and should be validated in larger populations.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12871-025-03168-x.
Keywords: Child; Congenital; Death; Paediatric; Prematurity.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Institutional Review Board of the University of Muenster, Germany (file reference 2019-398-f-S). Due to its retrospective nature, the requirement of written informed consent was waived by the Institutional Review Board. The study adheres to the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Prophylactic levosimendan for the prevention of low cardiac output syndrome and mortality in paediatric patients undergoing surgery for congenital heart disease.Cochrane Database Syst Rev. 2017 Aug 2;8(8):CD011312. doi: 10.1002/14651858.CD011312.pub3. Cochrane Database Syst Rev. 2017. PMID: 28770972 Free PMC article.
-
Thyroid hormone supplementation for the prevention of morbidity and mortality in infants undergoing cardiac surgery.Cochrane Database Syst Rev. 2004;(3):CD004220. doi: 10.1002/14651858.CD004220.pub2. Cochrane Database Syst Rev. 2004. PMID: 15266523
-
Prophylactic levosimendan for the prevention of low cardiac output syndrome and mortality in paediatric patients undergoing surgery for congenital heart disease.Cochrane Database Syst Rev. 2017 Mar 6;3(3):CD011312. doi: 10.1002/14651858.CD011312.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2017 Aug 02;8:CD011312. doi: 10.1002/14651858.CD011312.pub3. PMID: 28262914 Free PMC article. Updated.
-
Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants.Cochrane Database Syst Rev. 2017 Apr 11;4(4):CD011190. doi: 10.1002/14651858.CD011190.pub2. Cochrane Database Syst Rev. 2017. PMID: 28398697 Free PMC article.
-
Pre and peri-operative erythropoietin for reducing allogeneic blood transfusions in colorectal cancer surgery.Cochrane Database Syst Rev. 2009 Jan 21;(1):CD007148. doi: 10.1002/14651858.CD007148.pub2. Cochrane Database Syst Rev. 2009. PMID: 19160325
References
-
- Bhananker SM, Ramamoorthy C, Geiduschek JM, Posner KL, Domino KB, Haberkern CM, et al. Anesthesia-related cardiac arrest in children: update from the pediatric perioperative cardiac arrest registry. Anesth Analg. 2007;105:344–50. - PubMed
-
- Gobbo Braz L, Braz JR, Módolo NS, do Nascimento P, Brushi BA, Raquel de Carvalho L. Perioperative cardiac arrest and its mortality in children. A 9-year survey in a Brazilian tertiary teaching hospital. Paediatr Anaesth. 2006;16:860–6. - PubMed
LinkOut - more resources
Full Text Sources
