

Trajectories and dimensional phenotypes of depressive symptoms throughout pregnancy and postpartum in relation to prior premenstrual symptoms
- PMID: 40538355
- PMCID: PMC12257281
- DOI: 10.1192/bjp.2025.38
Trajectories and dimensional phenotypes of depressive symptoms throughout pregnancy and postpartum in relation to prior premenstrual symptoms
Abstract
Background: Sensitivity to ovarian hormone fluctuations can lead to mental distress during the luteal phase of the menstrual cycle, such as in premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD), and also during pregnancy and postpartum, as in perinatal depression (PND).
Aims: In two cohorts, we investigated the relationship between history of PMS/PMDD and PND symptoms. We also examined how premenstrual symptoms are associated with perinatal symptom trajectories and dimensional phenotypes of PND symptoms, which remains unidentified.
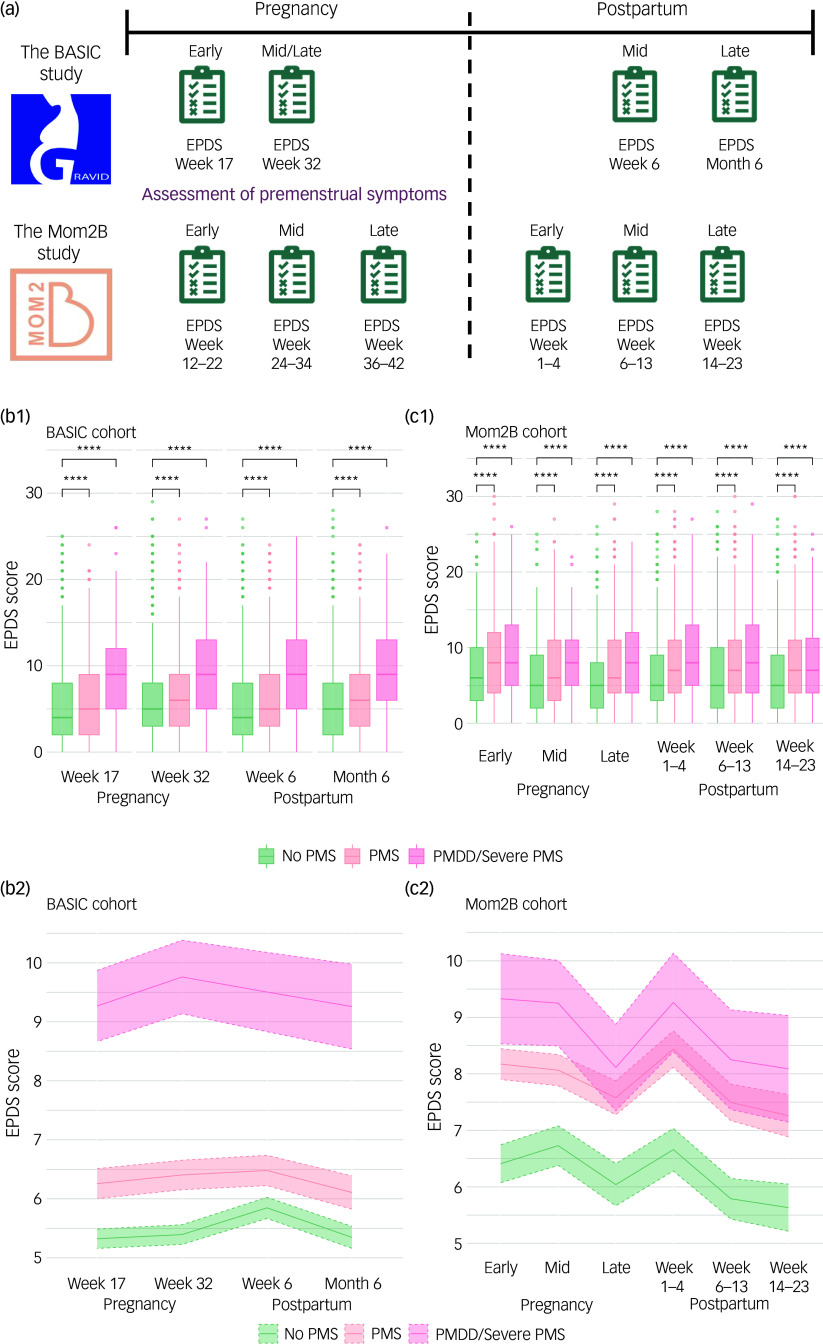
Method: From early pregnancy until 6 months postpartum, participants of two large longitudinal cohorts were followed using the Edinburgh Postnatal Depression Scale (EPDS). Premenstrual symptoms were self-reported retrospectively.
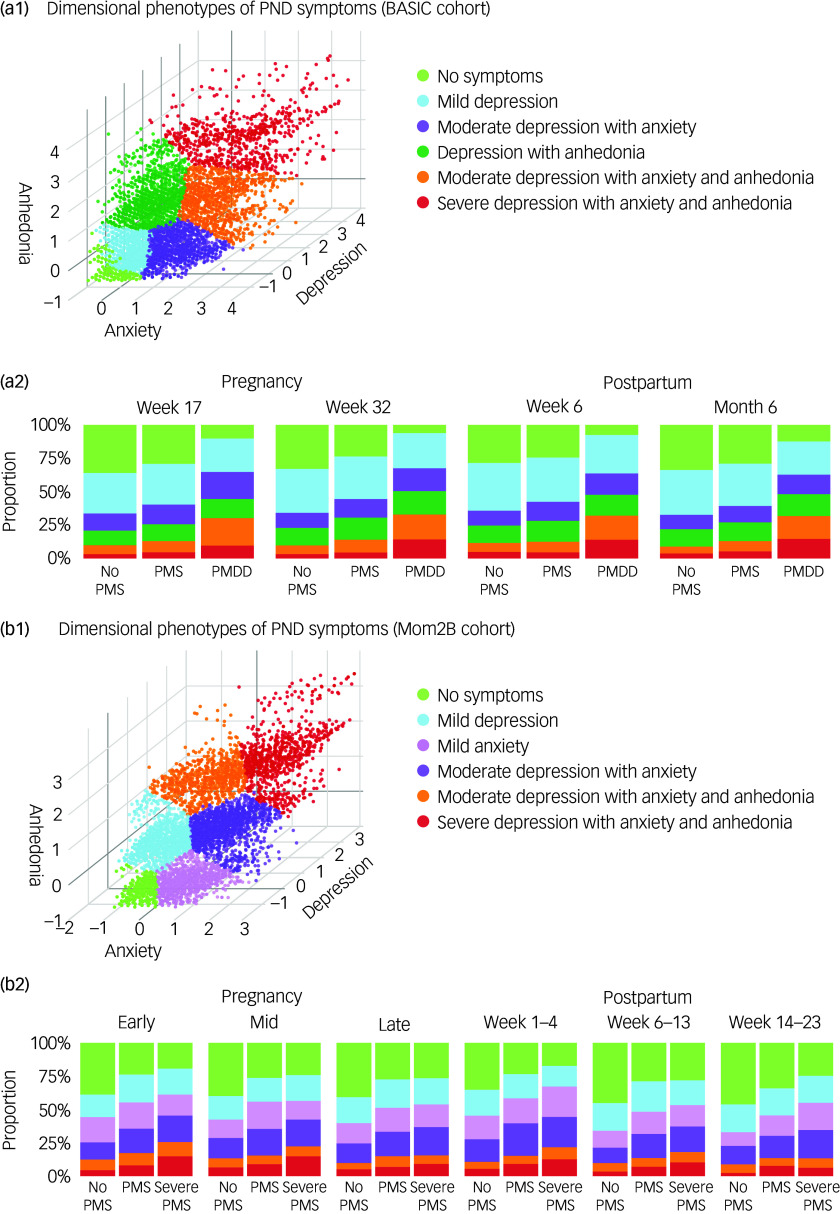
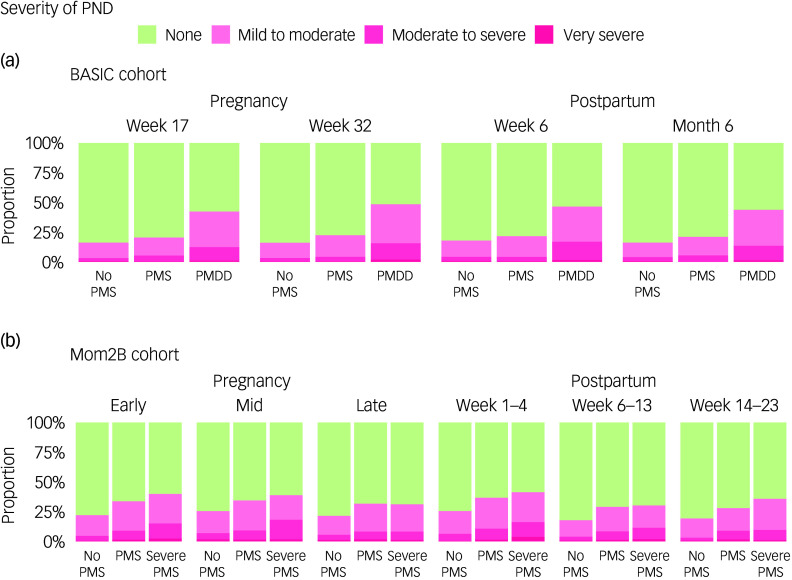
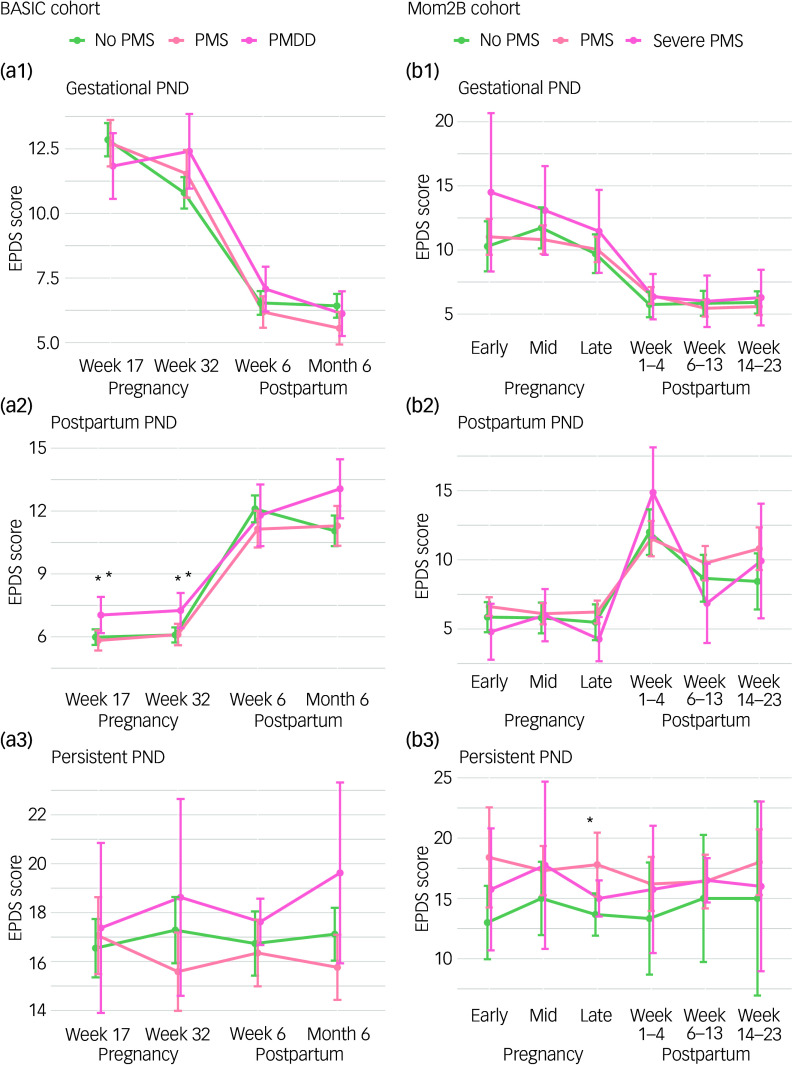
Results: Both pre-pregnancy PMS and PMDD were associated with higher EPDS scores across pregnancy and postpartum, even after adjustment for confounders. The odds of developing PND were higher among those reporting PMS and PMDD, ranging up to 1.68 (95% CI 1.25-2.29) (6-13 weeks postpartum) and 3.05 (95% CI 2.26-4.10) (late pregnancy) respectively for PMS and PMDD, throughout the perinatal period. Premenstrual symptomatology was associated more with certain PND trajectories based on the time of occurrence and persistence of symptoms. However, PND symptom severity did not differ depending on premenstrual symptomatology in any trajectory. Prior PMS/PMDD was associated with underlying dimensions of symptom constructs of PND, including severe and moderate symptoms of depressed mood, anxiety and anhedonia.
Conclusions: Women with a history of PMS/PMDD require coordinated care by psychiatrists, other mental health clinicians, midwives and gynaecologists during pregnancy as well as postpartum.
Keywords: Reproductive psychiatry; ovarian hormones; perinatal depression; premenstrual disorder; women.
Conflict of interest statement
I.S.-P. has occasionally served on advisory boards or acted as invited speaker at scientific meetings for Asarina Pharma, Bayer Health Care, Gedeon Richter, Peptonics, Shire/Takeda, Sandoz and Lundbeck A/S. These organisations were not involved in the design, conduct or reporting of the present research. E.C. is a member of the
Figures
Similar articles
-
Non-contraceptive oestrogen-containing preparations for controlling symptoms of premenstrual syndrome.Cochrane Database Syst Rev. 2017 Mar 3;3(3):CD010503. doi: 10.1002/14651858.CD010503.pub2. Cochrane Database Syst Rev. 2017. PMID: 28257559 Free PMC article.
-
Association between premenstrual dysphoric disorder and perinatal depression: a systematic review.Arch Womens Ment Health. 2022 Feb;25(1):61-70. doi: 10.1007/s00737-021-01177-6. Epub 2021 Aug 26. Arch Womens Ment Health. 2022. PMID: 34436653
-
Gonadotropin-releasing hormone (GnRH) analogues for premenstrual syndrome (PMS).Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD011330. doi: 10.1002/14651858.CD011330.pub2. Cochrane Database Syst Rev. 2025. PMID: 40492482 Review.
-
Selective serotonin reuptake inhibitors for premenstrual syndrome.Cochrane Database Syst Rev. 2013 Jun 7;2013(6):CD001396. doi: 10.1002/14651858.CD001396.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2024 Aug 14;8:CD001396. doi: 10.1002/14651858.CD001396.pub4. PMID: 23744611 Free PMC article. Updated.
-
The impact of comorbid premenstrual syndrome or premenstrual dysphoric disorder on the clinical characteristics of bipolar disorder among Han Chinese women.Arch Womens Ment Health. 2024 Feb;27(1):67-75. doi: 10.1007/s00737-023-01380-7. Epub 2023 Oct 24. Arch Womens Ment Health. 2024. PMID: 37874397
