

Chemotherapy plus bevacizumab with or without anti-programmed death 1 immunotherapy as the second-line therapy in colorectal cancer
- PMID: 40538515
- PMCID: PMC12175866
- DOI: 10.3748/wjg.v31.i21.106939
Chemotherapy plus bevacizumab with or without anti-programmed death 1 immunotherapy as the second-line therapy in colorectal cancer
Abstract
Background: Patients with microsatellite stable (MSS) metastatic colorectal cancer (mCRC) typically exhibit an immunosuppressive tumor microenvironment and demonstrate a low response rate to immunotherapy. Reports suggest that chemotherapy and anti-angiogenic therapy may have the potential to enhance the response to immunotherapy in these patients. This study aims to evaluate the effectiveness and safety of chemotherapy combined with bevacizumab with or without anti-programmed death 1 (PD-1) immunotherapy as the second-line regimen for MSS mCRC.
Aim: To evaluate the effectiveness and safety of chemotherapy combined with bevacizumab with or without anti-PD-1 immunotherapy as the second-line regimen for MSS mCRC.
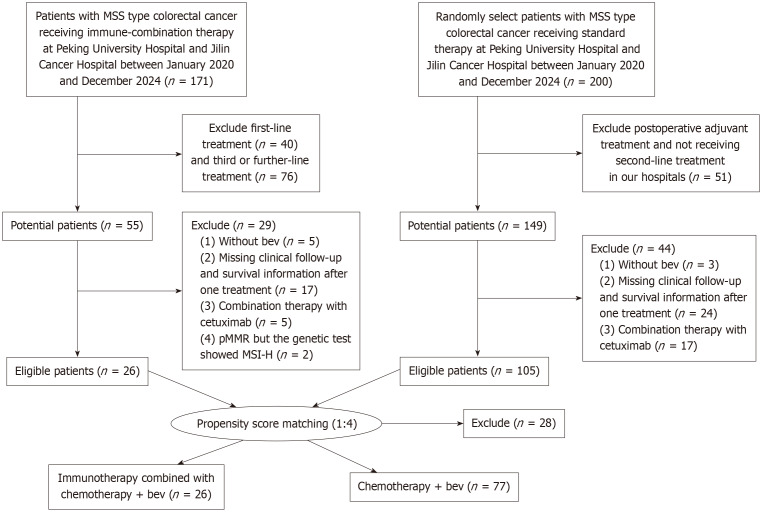
Methods: A retrospective analysis was conducted on patients with MSS mCRC diagnosed at Peking University First Hospital and Jilin Cancer Hospital from January 2020 to December 2024. The patients were divided into two groups: The experimental group receiving second-line chemotherapy combined with bevacizumab and anti-PD-1 immunotherapy, and the control group receiving chemotherapy combined with bevacizumab. Propensity score matching was applied to balance potential prognostic factors, including age, gender, Eastern Cooperative Oncology Group score, number of metastases, and primary tumor site. The progression-free survival, overall survival, disease control rate, objective response rate, and treatment-related adverse reactions were compared between the two groups. Kaplan-Meier analysis and log-rank test were used to compare survival outcomes. Inverse probability of treatment weighting was used for sensitivity analysis.
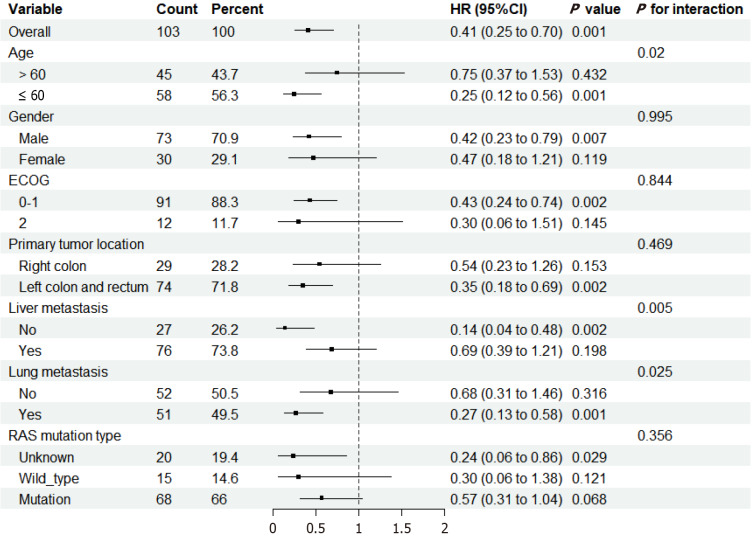
Results: Propensity score matching resulted in 103 matched eligible patients. The median follow-up period was 13.9 months in the matched cohort. The objective response rate was 11.5% and 9% for the experimental and control groups, respectively (P = 0.710), while the disease control rate was 76.9% and 53.2%, respectively (P = 0.058). The median progression-free survival in the experimental group was 8.27 months [95% confidence interval (CI): 6.7-14.7 months], significantly higher than that in the control group, which was 4.63 months (95%CI: 3.9-5.67 months) (hazard ratio = 0.4143, 95%CI: 0.2462-0.6972, P = 0.00066). There was a trend towards the higher median overall survival in the experimental group compared to the control group (hazard ratio = 0.4504, 95%CI: 0.1897-1.07, P = 0.064). The incidences of adverse events were similar between the two groups.
Conclusion: Compared with the standard second-line chemotherapy combined with bevacizumab regimen, second-line therapy that combines chemotherapy with bevacizumab and anti-PD-1 immunotherapy has demonstrated promising efficacy in the treatment of MSS mCRC, while exhibiting a similar safety profile.
Keywords: Immune checkpoint inhibitors; Metastatic colorectal cancer; Microsatellite stable; Programmed death 1; RAS mutation.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures





Similar articles
-
Real-world comparison of chemotherapy plus bevacizumab with or without immunotherapy as first-line therapy in colorectal cancer.World J Gastroenterol. 2025 Jun 28;31(24):108298. doi: 10.3748/wjg.v31.i24.108298. World J Gastroenterol. 2025. PMID: 40599189 Free PMC article.
-
Targeted therapy combined with immunotherapy vs trifluridine/tipiracil with bevacizumab as late-line therapy in metastatic colorectal cancer.World J Gastroenterol. 2025 Aug 7;31(29):109947. doi: 10.3748/wjg.v31.i29.109947. World J Gastroenterol. 2025. PMID: 40809924 Free PMC article.
-
Real world effectiveness of chemotherapy plus bevacizumab with immunotherapy in colorectal cancer.Sci Rep. 2025 Aug 9;15(1):29170. doi: 10.1038/s41598-025-13701-0. Sci Rep. 2025. PMID: 40783607 Free PMC article.
-
Evaluation of the efficacy and safety of first- and second-line immunotherapy in patients with metastatic colorectal cancer: a systematic review and network meta-analysis based on randomized controlled trials.Front Immunol. 2024 Sep 18;15:1439624. doi: 10.3389/fimmu.2024.1439624. eCollection 2024. Front Immunol. 2024. PMID: 39359729 Free PMC article.
-
Comparison of efficacy and safety of PD-1/PD-L1 combination therapy in first-line treatment of advanced NSCLC: an updated systematic review and network meta-analysis.Clin Transl Oncol. 2024 Oct;26(10):2488-2502. doi: 10.1007/s12094-024-03442-3. Epub 2024 Apr 16. Clin Transl Oncol. 2024. PMID: 38625495
References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–263. - PubMed
-
- Tournigand C, André T, Achille E, Lledo G, Flesh M, Mery-Mignard D, Quinaux E, Couteau C, Buyse M, Ganem G, Landi B, Colin P, Louvet C, de Gramont A. FOLFIRI Followed by FOLFOX6 or the Reverse Sequence in Advanced Colorectal Cancer: A Randomized GERCOR Study. J Clin Oncol. 2023;41:3469–3477. - PubMed
-
- Bennouna J, Hiret S, Bertaut A, Bouché O, Deplanque G, Borel C, François E, Conroy T, Ghiringhelli F, des Guetz G, Seitz JF, Artru P, Hebbar M, Stanbury T, Denis MG, Adenis A, Borg C. Continuation of Bevacizumab vs Cetuximab Plus Chemotherapy After First Progression in KRAS Wild-Type Metastatic Colorectal Cancer: The UNICANCER PRODIGE18 Randomized Clinical Trial. JAMA Oncol. 2019;5:83–90. - PMC - PubMed
-
- Hecht JR, Cohn A, Dakhil S, Saleh M, Piperdi B, Cline-Burkhardt M, Tian Y, Go WY. SPIRITT: A Randomized, Multicenter, Phase II Study of Panitumumab with FOLFIRI and Bevacizumab with FOLFIRI as Second-Line Treatment in Patients with Unresectable Wild Type KRAS Metastatic Colorectal Cancer. Clin Colorectal Cancer. 2015;14:72–80. - PubMed
-
- Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, Seligmann J, De Baere T, Osterlund P, Yoshino T, Martinelli E ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34:10–32. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
