

Late Pancreatic Metastasis From Papillary Thyroid Carcinoma Diagnosed by Endoscopic Ultrasound-Guided Tissue Acquisition
- PMID: 40538612
- PMCID: PMC12175758
- DOI: 10.31486/toj.24.0115
Late Pancreatic Metastasis From Papillary Thyroid Carcinoma Diagnosed by Endoscopic Ultrasound-Guided Tissue Acquisition
Abstract
Background: Papillary thyroid carcinoma, the most common differentiated thyroid cancer, has an indolent clinical course and a good prognosis. Metastases to the gastrointestinal tract account for <1% of all distant metastases, and the pancreas is an extremely rare site for metastasis from thyroid cancer.
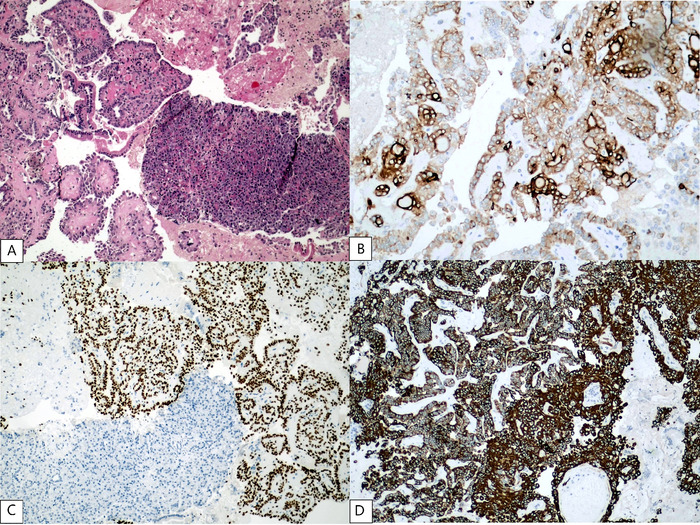
Case report: We report the case of a patient who developed a pancreatic metastasis from a classic variant papillary thyroid carcinoma 11 years after total thyroidectomy, cervical lymphadenectomy, and radioactive iodine ablation. The patient experienced increased thyroglobulin levels, and abdominal computed tomography scan revealed a lesion in the uncinate process of the pancreas. Tissue samples obtained by endoscopic ultrasound-guided biopsy were positive for thyroglobulin and thyroid transcription factor 1. Because the patient was not a candidate for surgery, the metastatic lesion was not iodine-avid, and tyrosine kinase inhibitors could not be offered because of tumor-related symptoms, the patient was treated with stereotactic body radiotherapy only. The patient died almost 2 years after the diagnosis of metastatic papillary thyroid carcinoma to the pancreas (13 years after total thyroidectomy for the primary cancer).
Conclusion: If pancreatic lesions are discovered during regular follow-up of patients who have previously been treated for papillary thyroid carcinoma, pancreatic metastasis must be considered, and imaging procedures other than whole-body iodine scintigraphy are required. Histopathology and iodine avidity will define the best therapeutic strategy. Radioactive iodine ablation should be considered for iodine-avid metastases, and surgery or tyrosine kinase inhibitors are promising options for non-iodine-avid lesions.
Keywords: Endoscopic ultrasound-guided fine needle aspiration; neoplasm metastasis; pancreatic neoplasms; thyroid cancer–papillary.
©2025 by the author(s); Creative Commons Attribution License (CC BY).
Conflict of interest statement
The authors have no financial or proprietary interest in the subject matter of this article.
Figures


Similar articles
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Imaging modalities for characterising focal pancreatic lesions.Cochrane Database Syst Rev. 2017 Apr 17;4(4):CD010213. doi: 10.1002/14651858.CD010213.pub2. Cochrane Database Syst Rev. 2017. PMID: 28415140 Free PMC article.
-
Transabdominal ultrasound and endoscopic ultrasound for diagnosis of gallbladder polyps.Cochrane Database Syst Rev. 2018 Aug 15;8(8):CD012233. doi: 10.1002/14651858.CD012233.pub2. Cochrane Database Syst Rev. 2018. PMID: 30109701 Free PMC article.
-
Synchronous or metachronous presentation of pancreatic neuroendocrine tumor versus secondary lesion to pancreas in patients affected by renal cell carcinoma. Systematic review.Semin Oncol. 2022 Dec;49(6):476-481. doi: 10.1053/j.seminoncol.2023.01.007. Epub 2023 Feb 2. Semin Oncol. 2022. PMID: 36759234
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
References
-
- Sugimura H, Tamura S, Kodama T, Kakitsubata Y, Asada K, Watanabe K. Metastatic pancreas cancer from the thyroid; clinical imaging mimicking non functioning islet cell tumor. Radiat Med. 1991;9(5):167-169. - PubMed
Publication types
LinkOut - more resources
Full Text Sources