

Hyperspectral abdominal laparoscopy with real-time quantitative tissue oxygenation imaging: a live porcine study
- PMID: 40538619
- PMCID: PMC12176765
- DOI: 10.3389/fmedt.2025.1549245
Hyperspectral abdominal laparoscopy with real-time quantitative tissue oxygenation imaging: a live porcine study
Abstract
Background: Ischaemia is a critical complication, and can result in poor surgical outcomes. While intra-operative overt ischaemia can be perceived with the naked eye, timely recognition of borderline perfusion can prevent post-operative ischaemic complications, which is particularly relevant for colorectal anastomoses. Consequently, there is a clinical need for new technologies to intra-operatively assess tissue oxygenation (indicative of end organ perfusion), with minimal disruption to the surgical workflow. Here we present a hyperspectral imaging (HSI) system for laparoscopic surgery. This system provides live, easy to interpret, tissue oxygenation (StO2) maps with associated quantitative values.
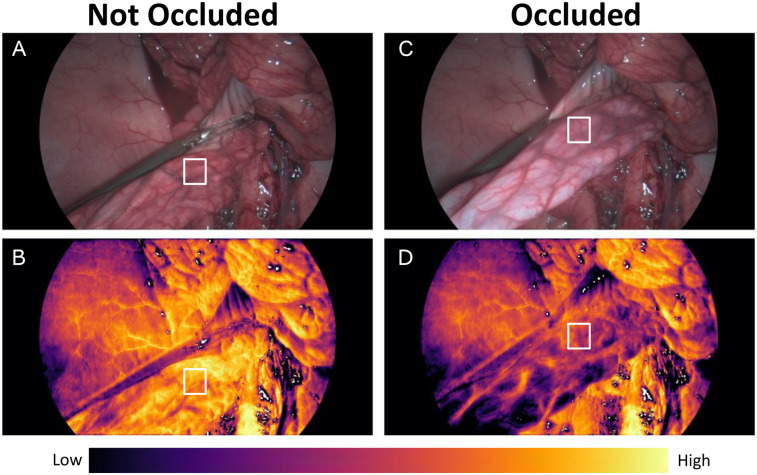
Methods: White light view and tissue oxygenation maps were reconstructed from a protoype laparoscopic Hyperspectral Surgical System (HSS). First, in a live porcine model (55 kg female), the mesentery of a small bowel loop was temporarily occluded with a laparoscopic grasper, then released whilst being imaged with HSI. The quantitative StO2 values obtained from the HSS were compared with those of a non-invasive tissue oximetry probe (Moor VMS-Oxy, Moor Instruments Ltd, United Kingdom). Secondly, mimicking a laparoscopic colon resection and anastomosis, the colorectal junction was mobilised laparoscopically, exteriorised, transected, anastomosed and repositioned in the abdominal cavity. In order to compare healthy and ischaemic colon, the distal part was intentionally devascularised. Tissue oxygenation maps were compared with indocyanine green fluorescence angiography (ICG-FA) of the anastomotic region.
Results: The HSS was used as the primary scope to complete a laparoscopic colorectal anastomosis, providing a simultaneous white light view and hyperspectral information. Quantitative results from small bowel imaging were shown to correlate with measurements from the superficial tissue oximetry probe. Real-time tissue oxygenation maps were shown to visually correlate with ICG-FA.
Conclusion: The HSS can guide laparoscopic surgical procedures whilst providing visual and quantitative tissue oxygenation information in a live animal model. This paves the way for further studies to assess clinical applications.
Keywords: StO2; anastomosis; hyperspectral imaging; laparoscopy; minimally invasive surgery; tissue oxygenation.
© 2025 MacCormac, Horgan, Waterhouse, Noonan, Janatka, Miles, Jacobs, Dockerill, Trotouin, Schizas, Seeliger, Ourselin, Ebner, Vercauteren and Shapey.
Conflict of interest statement
The authors declare that the research was conducted in collaboration between Hypervision Surgical and King’s College London. Authors ME, PN, MJ, CH, TT, JJ, CD, DW are all paid employees of Hypervision Surgical Ltd. ME, TV, SO and JS are shareholders and co-founders of Hypervision Surgical Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




 rectum and well perfused
rectum and well perfused  colon. (A) HSI-generated RGB. (B) Near-infrared (NIR) enabled laparoscope RGB. (C) HSI-generated StO2 map. (D) NIR overlay of the same anastomotic region. Different viewpoints of the anastomosis are due to imaging via different ports to accommodate both the HSS and laparoscope (Ele Vision).
colon. (A) HSI-generated RGB. (B) Near-infrared (NIR) enabled laparoscope RGB. (C) HSI-generated StO2 map. (D) NIR overlay of the same anastomotic region. Different viewpoints of the anastomosis are due to imaging via different ports to accommodate both the HSS and laparoscope (Ele Vision).
Similar articles
-
Indocyanine green near-infrared fluorescence bowel perfusion assessment to prevent anastomotic leakage in minimally invasive colorectal surgery (AVOID): a multicentre, randomised, controlled, phase 3 trial.Lancet Gastroenterol Hepatol. 2024 Oct;9(10):924-934. doi: 10.1016/S2468-1253(24)00198-5. Epub 2024 Aug 13. Lancet Gastroenterol Hepatol. 2024. PMID: 39151436 Clinical Trial.
-
ICG-augmented hyperspectral imaging for visualization of intestinal perfusion compared to conventional ICG fluorescence imaging: an experimental study.Int J Surg. 2023 Dec 1;109(12):3883-3895. doi: 10.1097/JS9.0000000000000706. Int J Surg. 2023. PMID: 38258996 Free PMC article.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.Health Technol Assess. 2006 Nov;10(45):1-141, iii-iv. doi: 10.3310/hta10450. Health Technol Assess. 2006. PMID: 17083853
-
Laparoscopic surgery for elective abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 May 4;5(5):CD012302. doi: 10.1002/14651858.CD012302.pub2. Cochrane Database Syst Rev. 2017. PMID: 28471523 Free PMC article.
-
Endovascular treatment for ruptured abdominal aortic aneurysm.Cochrane Database Syst Rev. 2017 May 26;5(5):CD005261. doi: 10.1002/14651858.CD005261.pub4. Cochrane Database Syst Rev. 2017. PMID: 28548204 Free PMC article.
References
-
- Murray AC, Lourenco T, De Verteuil R, Hernández RA, Fraser MF, McKinley AJ, et al. Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation. Health Technol Assess (Rockv). (2006) 10(45):1–141, iii-iv. 10.3310/hta10450 - DOI - PubMed
LinkOut - more resources
Full Text Sources