

Reduced hemolytic complement activity in the classical pathway (CH50) is a risk factor for poor clinical outcomes of patients with infections: a retrospective analysis of health insurance claims in Japan
- PMID: 40539044
- PMCID: PMC12176544
- DOI: 10.3389/fimmu.2025.1601690
Reduced hemolytic complement activity in the classical pathway (CH50) is a risk factor for poor clinical outcomes of patients with infections: a retrospective analysis of health insurance claims in Japan
Abstract
Purpose: To evaluate whether low CH50 (a comprehensive measure of hemolytic activity of the classical complement pathway) is associated with infection-related coagulopathy, organ dysfunction, and poor clinical outcomes.
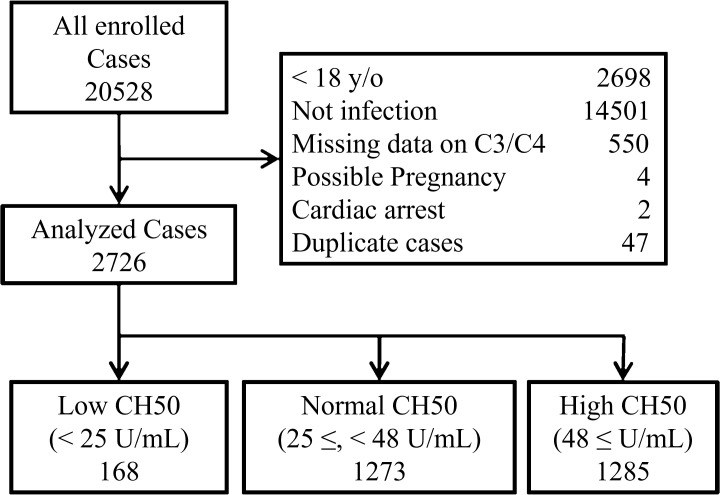
Methods: This was a retrospective study using Japanese health insurance claim data (2014-2023). Adult patients whose CH50 values were measured within one week of admission were included. We divided the patients into three groups based on the normal CH50 range: Low CH50 (< 25 U/mL; n=168), Normal CH50 (25 ≤, < 48 U/mL; n=1273), and High CH50 (48 ≤ U/mL; n=1285).
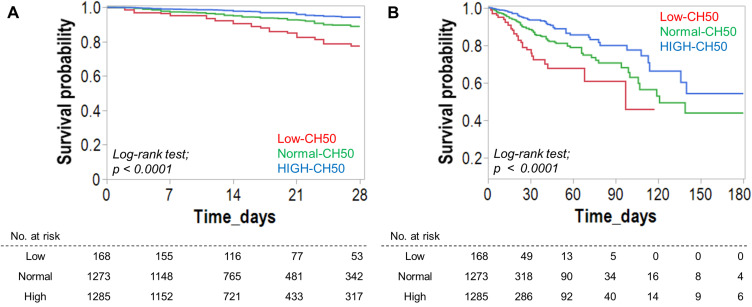
Results: Of 2,726 patients who met the inclusion criteria, logistic regression models demonstrated that decreased CH50 is a significant predictor of 180-day mortality (OR: 0.98-0.99). Cumulative survival rates in the Low CH50 group at 28 days and 180 days were both unfavorable (both p < 0.0001, Log-rank test). CH50 was significantly inversely correlated with SOFA, SIC, ISTH-overt DIC, and JAAM-2 DIC scores, and was also correlated with C3 and C4 levels. Diminished CH50 may be particularly useful in diagnosing SIC (specificity; 79.2%) and excluding ISTH-overt DIC (sensitivity; 90.5%). Moreover, patients with low levels of both CH50 and C3 had an extremely high mortality rate (25.0%).
Conclusion: Low CH50 after infection is not only significantly associated with multiple organ failure and coagulopathy but is also an independent risk factor for poor prognosis. Complement activation after infection may help to avert organ damage and to improve clinical outcomes.
Keywords: CH50; coagulopathy; health insurance claims database; infection; outcome.
Copyright © 2025 Koami, Furukawa, Hirota, Sasaki, Ogawa, Matsuoka, Shinada, Nakayama, Sakurai, Iwanaga, Onohara, Narumi, Koba, Mori, Umemura, Yamakawa, Okamoto and Sakamoto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. HK investigated and established the research methodology. HK, KY and YU managed the project. YS supervised the entire study. YF, KY and YU conducted the validation of the study. Data curation, formal analysis, visualization of the study and writing of the original draft were performed by HK. Review and editing the manuscript were performed by YF, YH, AS, HO, AM, KS, KN, RS, SI, TO, SN, MK, HM, YU, KY, KO, and YS. All authors revised the manuscript for important intellectual content. All authors read and approved the final version of the manuscript.
Figures
Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous