

FERTILITY CARE IN LOW- AND MIDDLE-INCOME COUNTRIES: Public sector access to medically assisted reproduction in South Africa: a case study
- PMID: 40539898
- PMCID: PMC12257605
- DOI: 10.1530/RAF-24-0072
FERTILITY CARE IN LOW- AND MIDDLE-INCOME COUNTRIES: Public sector access to medically assisted reproduction in South Africa: a case study
Abstract
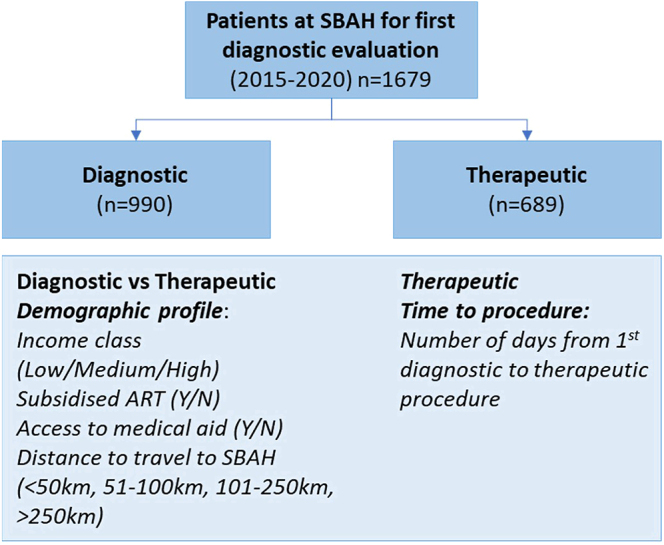
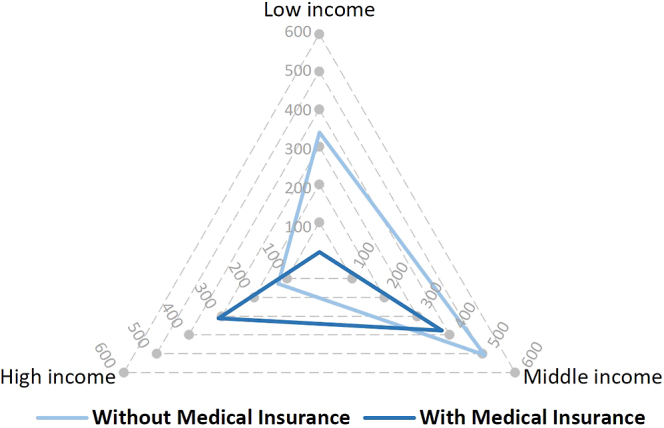
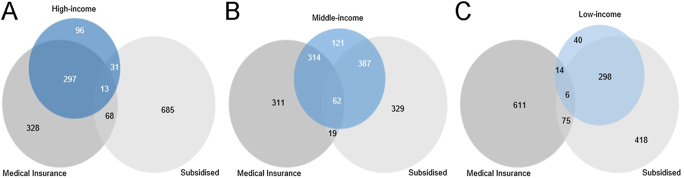
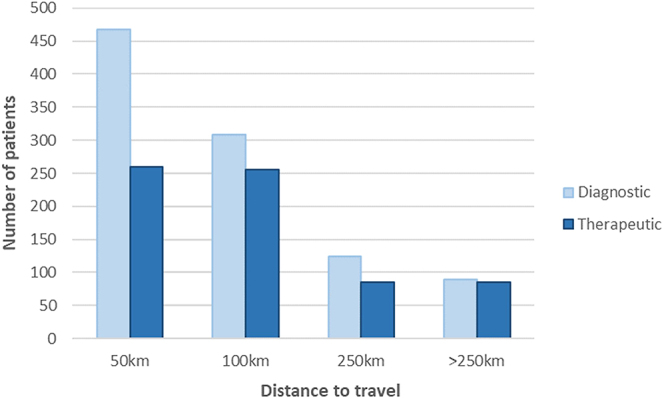
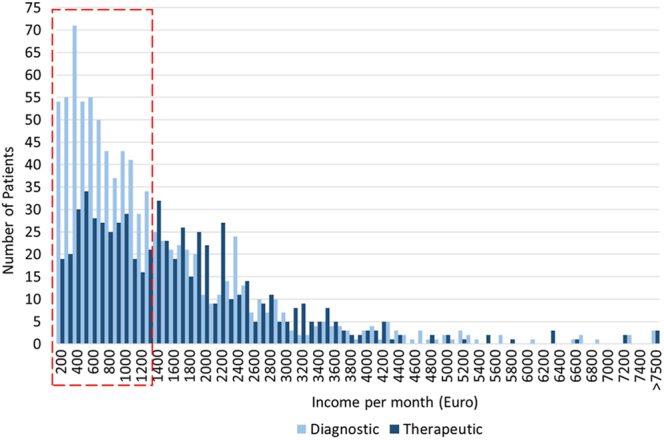
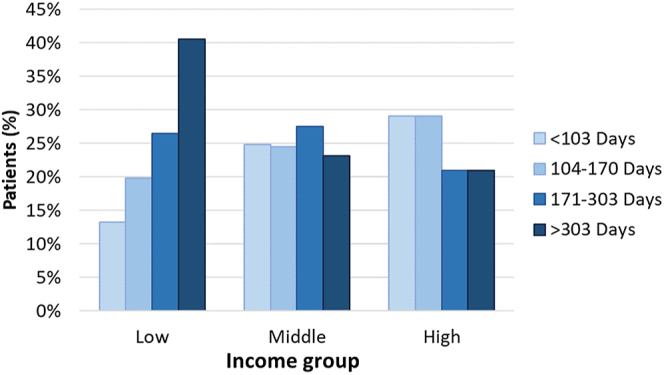
Abstract: In South Africa, approximately 10% of the calculated need for medically assisted reproduction is being met due to limited access and unequal availability of these services. To facilitate understanding of challenges associated with access to assisted reproduction, a retrospective case study spanning 6 years was performed at one public sector hospital in South Africa offering these services. Demographic profiles, including income, region of residency and access to medical insurance, of patients seeking assistance to become pregnant were investigated. Patients were categorised as those who underwent diagnostic investigations only vs those who returned for therapeutic procedures, and the difference in demographic profiles between the two groups was determined. This investigation showed that patients from the lower-income classification group, without medical insurance, tend to return for therapeutic procedures less often than those with a higher income and medical insurance, even though these low-income patients qualify for a therapeutic procedure subsidy. An inverse relationship existed where patient numbers decreased as their travel distance increased, but patients who were required to travel further for assisted reproductive therapy tended to return for these procedures more often than patients who resided closer to the medical facility. In conclusion, access to medically assisted reproduction facilities is critically undersupplied and limited in the region. In order to ease the travel distance of patients, alternative primary diagnostic routes with accessible clinics are needed. In addition, costs of therapeutic procedures in the public sector should be re-evaluated to be offered at affordable rates for marginalised patients.
Lay summary: In South Africa, about 10% of patients who need assistance to become pregnant are being helped. To better understand this phenomenon, researchers considered information about patients from a public sector hospital in South Africa. This includes how much money the patients earned, how far they travelled to the hospital and whether they had medical insurance. The patients were grouped into those who requested initial investigations but never returned for treatments, and those who returned for medical treatment. The differences between these groups were then evaluated. The research showed that people with less money tend to abandon further treatment more often, or take longer to return, than those with more money. The conclusion drawn is that assisted reproductive therapy is too expensive and that more IVF clinics are needed, using cheaper and simpler procedures of the same quality.
Keywords: LMIC; MAR; access; assisted reproduction; developing countries; patient demographics; treatment progression.
Conflict of interest statement
The following interests are relevant: the data presented are part of a larger study performed during the principal author’s PhD research. All the authors are associated with the Walking Egg non-profit organisation. W Ombelet is an Associate Editor of
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
