

International Consensus Histopathological Criteria for Subtyping Idiopathic Multicentric Castleman Disease Based on Machine Learning Analysis
- PMID: 40540535
- PMCID: PMC12326216
- DOI: 10.1002/ajh.27743
International Consensus Histopathological Criteria for Subtyping Idiopathic Multicentric Castleman Disease Based on Machine Learning Analysis
Abstract
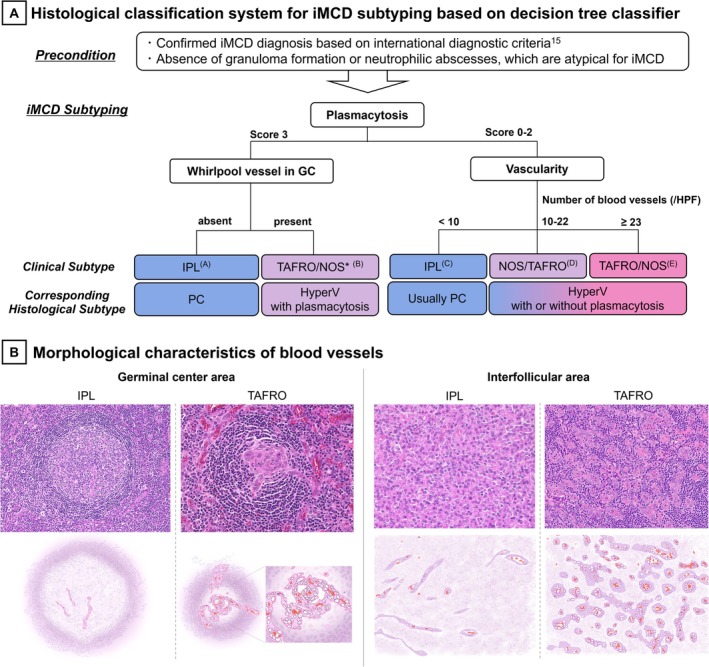
Idiopathic multicentric Castleman disease (iMCD) is a rare lymphoproliferative disorder classified into three recognized clinical subtypes-idiopathic plasmacytic lymphadenopathy (IPL), TAFRO, and NOS. Although clinical criteria are available for subtyping, diagnostically challenging cases with overlapping histopathological features highlight the need for an improved classification system integrating clinical and histopathological findings. We aimed to develop an objective histopathological subtyping system for iMCD that closely correlates with the clinical subtypes. Excisional lymph node specimens from 94 Japanese iMCD patients (54 IPL, 28 TAFRO, 12 NOS) were analyzed for five key histopathological parameters: germinal center (GC) status, plasmacytosis, vascularity, hemosiderin deposition, and "whirlpool" vessel formation in GC. Using hierarchical clustering, we visualized subgroups and developed a machine learning-based decision tree to differentiate the clinical subtypes and validated it in an external cohort of 12 patients with iMCD. Hierarchical cluster analysis separated the IPL and TAFRO cases into mutually exclusive clusters, whereas the NOS cases were interspersed between them. Decision tree modeling identified plasmacytosis, vascularity, and whirlpool vessel formation as key features distinguishing IPL from TAFRO, achieving 91% and 92% accuracy in the training and test sets, respectively. External validation correctly classified all IPL and TAFRO cases, confirming the reproducibility of the system. Our histopathological classification system closely aligns with the clinical subtypes, offering a more precise approach to iMCD subtyping. It may enhance diagnostic accuracy, guide clinical decision-making for predicting treatment response in challenging cases, and improve patient selection for future research. Further validation of its versatility and clinical utility is required.
Keywords: clinical subtype; histopathological criteria; idiopathic multicentric castleman disease; lymphoproliferative disease; machine‐learning.
© 2025 The Author(s). American Journal of Hematology published by Wiley Periodicals LLC.
Conflict of interest statement
E.O. has served as a consultant for Recordati Rare Diseases and as an expert on the advisory board for CSL Behring. D.C.F. has received research funding and consulting fees from Recordati Rare Diseases. The remaining authors declare no competing financial interests. F.v.R. has served on advisory boards for Adicet Bio, Bristol Myers Squibb, Castleman Disease Collaborative Network, EUSA Pharma, GlaxoSmithKline, Janssen Pharmaceuticals Inc., Kite Pharma, Secura Bio, Myeloma360, and Recordati. Additionally, F.v.R. has received donated study drugs for clinical trials from Pfizer.
Figures



References
-
- Tumour‐like lesions with B‐cell predominance , WHO Classification of Haematolymphoid Tumours, 5th ed. (International Agency for Research on Cancer (IARC), 2024).
-
- Lang E. and van Rhee F., “Idiopathic Multicentric Castleman Disease: An Update in Diagnosis and Treatment Advances,” Blood Reviews 64 (2024): 101161. - PubMed
-
- Mohri S. Mori, N., Uchida T., and Shimamine T., “Idiopathic Plasmacytic Lymphadenopathy With Polyclonal Hyperimmunoglobulinemia: A Syndrome Related to Giant Lymph Node Hyperplasia of Plasma Cell Type [in Japanese],” Japanese Journal of Sociological Research 20, no. suppl (1980): 55–65.
-
- Kojima M., Nakamura N., Tsukamoto N., et al., “Clinical Implications of Idiopathic Multicentric Castleman Disease Among Japanese: A Report of 28 Cases,” International Journal of Surgical Pathology 16 (2008): 391–398. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
