

Global Trends in Ischemic Heart Disease-Related Mortality From 2000 to 2019
- PMID: 40540773
- PMCID: PMC12221645
- DOI: 10.1016/j.jacadv.2025.101904
Global Trends in Ischemic Heart Disease-Related Mortality From 2000 to 2019
Abstract
Background: Ischemic heart disease (IHD) remains one of the leading causes of morbidity and mortality across the globe, and disparities exist based on sex and geographic region.
Objectives: This study investigates global trends in IHD mortality and examines disparities based on sex and geographic regions.
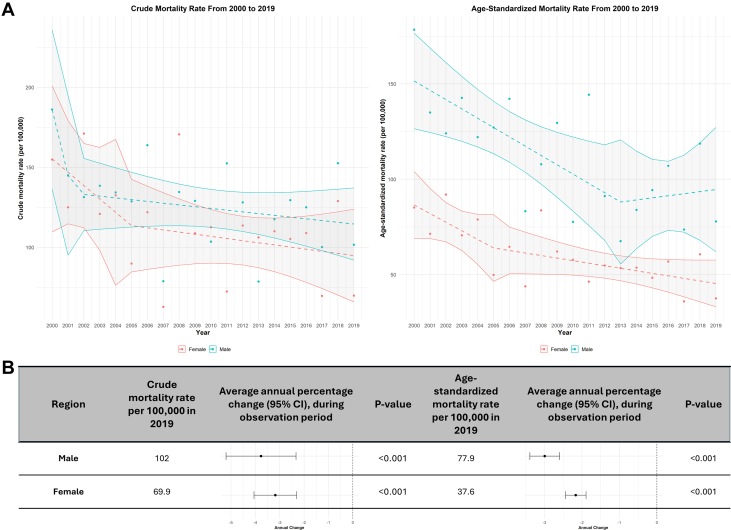
Methods: IHD mortality data from 105 countries were obtained from the World Health Organization Mortality Database. Crude mortality rates (CMRs) and age-standardized mortality rates (ASMRs) per 100,000 individuals were calculated, with average annual percentage change (AAPC) analyzed using joinpoint regression. Regional and sex-specific trends were assessed using stratified analyses of CMR and ASMR.
Results: Globally, CMR declined from 138 per 100,000 (95% CI: 131-145) in 2000 to 106 per 100,000 (95% CI: 102-114) in 2019 (AAPC: -1.79, 95% CI: -1.93 to -1.66). Similarly, ASMR declined from 104 per 100,000 (95% CI: 99-108) to 65.5 (95% CI: 62-69) in 2019 per 100,000 (AAPC: -2.16, 95% CI: -2.13 to -2.20). Regionally, CMRs decreased in Oceania, Europe, and North America, while they rose in Asia, Africa, and Central and South America. ASMRs declined worldwide except in Africa (AAPC: 1.33, 95% CI: 1.30-1.36). Males showed higher mortality than females, but both sexes demonstrated decreasing trends, with males having a steeper decline. In age groups across all regions, Africa showed an upward trend, while other regions demonstrated declines.
Conclusions: While global IHD mortality has declined from 2000 to 2019, disparities by geographic region and sex persist. Implementing targeted health awareness programs and collaborative global health efforts are crucial for addressing these inequalities.
Keywords: cardiovascular pathology; global trends; ischemic heart disease; mortality.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding support and author disclosures Dr Fonarow has consulted for Abbott, Amgen, AstraZeneca, Bayer, Boehinger Ingelheim, Cytokinetics, Eli Lilly, Johnson & Johnson, Medtronic, Merck, Novartis, and Pfizer. Dr Banach has received research grant(s)/support from Amgen, Daiichi Sankyo, Mylan/Viatris, and Sanofi and has served as a speaker and consultant for Adamed, Amgen, Daiichi Sankyo, Esperion, Exceed Pharma, Kogen, KRKA, Menarini, Mylan, Novartis, Novo Nordisk, Pfizer, Polpharma, Sanofi-Aventis, Servier, Teva, and Zentiva. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- GBD 2021 Diseases and Injuries Collaborators Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease study 2021. Lancet. 2024;403(10440):2133–2161. doi: 10.1016/S0140-6736(24)00757-8. - DOI - PMC - PubMed
-
- World Health Organization WHO Mortality Database. Accessed September 10, 2024 https://platform.who.int/mortality/themes/theme-details/MDB/all-causes
-
- Barco S., Valerio L., Ageno W., et al. Age-sex specific pulmonary embolism-related mortality in the USA and Canada, 2000-18: an analysis of the WHO Mortality Database and of the CDC multiple cause of death database. Lancet Respir Med. 2021;9(1):33–42. doi: 10.1016/S2213-2600(20)30417-3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
