

Self-reported disability trajectories and their predictors among patients receiving care by physical therapists for musculoskeletal conditions: a retrospective analysis of registry data
- PMID: 40541444
- PMCID: PMC12185884
- DOI: 10.1136/bmjopen-2025-099315
Self-reported disability trajectories and their predictors among patients receiving care by physical therapists for musculoskeletal conditions: a retrospective analysis of registry data
Abstract
Objectives: To identify clustered trajectories of self-reported disability following the initiation of care by a physical therapist in outpatient orthopaedic settings and to determine baseline factors that distinguish between different trajectories.
Design: Retrospective cohort study using electronic health record and patient-reported outcome data.
Setting: Data were extracted from the ATI Patient Outcomes Registry, encompassing patient encounters from over 900 ATI outpatient physical therapy clinics in 26 states across the USA.
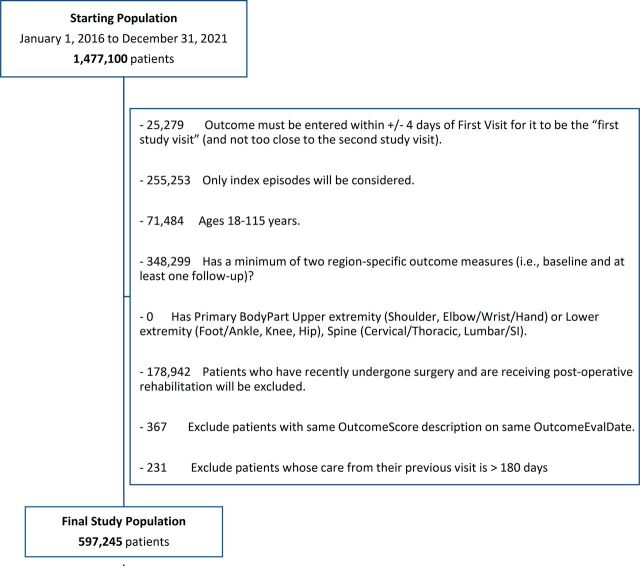
Participants: Patients receiving physical therapy after surgery were excluded. The final analytical sample included 597 245 unique patients initiating care between 1 January 2016 and 31 December 2021 for management of a spine, upper extremity or lower extremity musculoskeletal condition.
Interventions: Patients received treatments which could include strengthening and range of motion exercises, manual therapy, education, functional training and pain-relieving modalities.
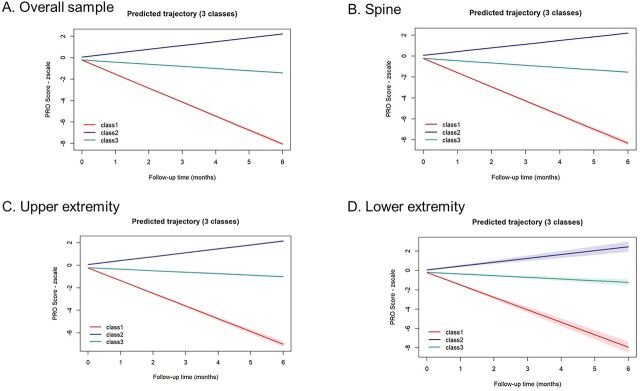
Primary and secondary outcome measures: The primary outcome was trajectory of self-reported, joint-specific disability measure scores up to 6 months following initial evaluation.
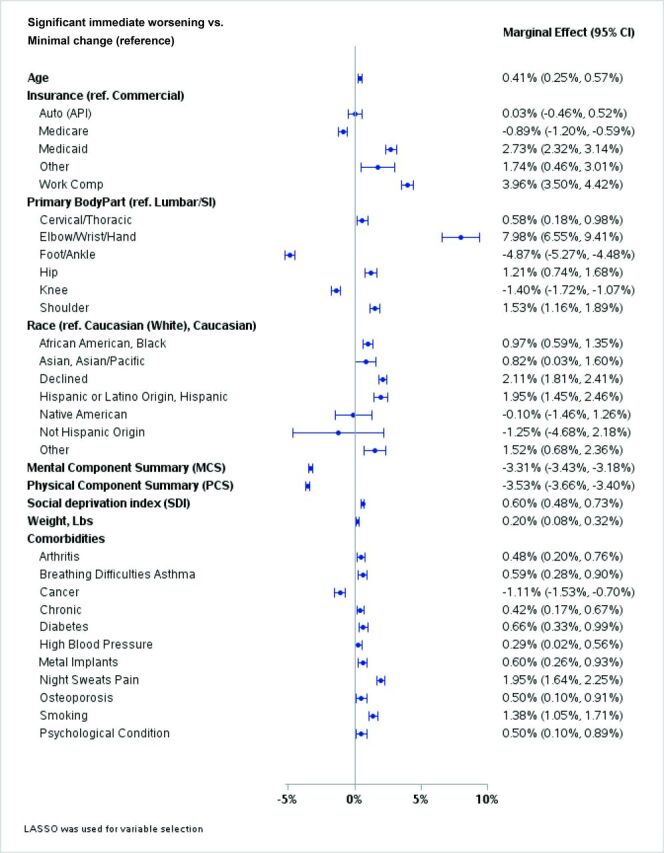
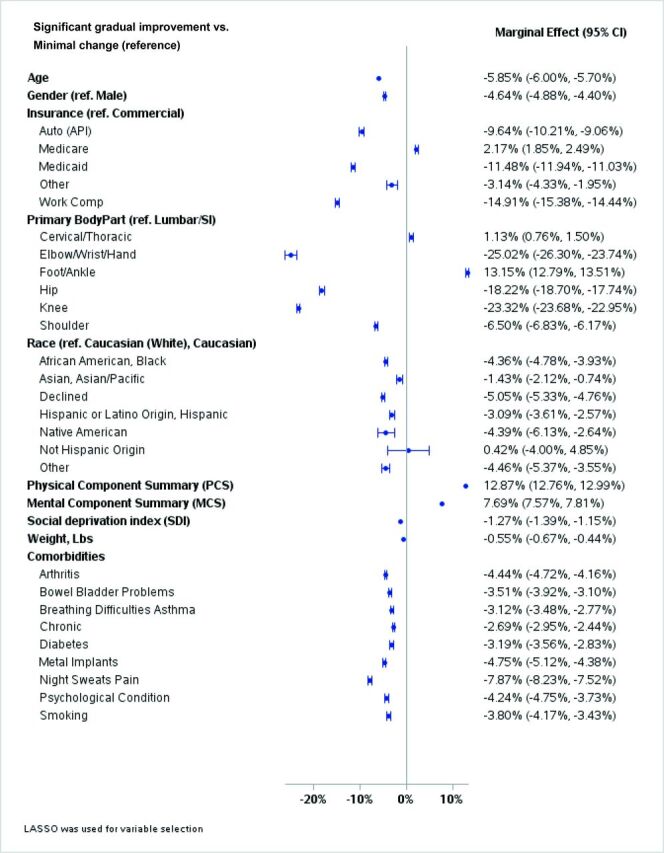
Results: Three distinct disability trajectory clusters were identified (proportion of sample; beta coefficient (95% CI)): significant immediate worsening (3.4%; -1.31 (-1.33, -1.28)), significant gradual improvement (61.4%; (0.36 (0.35, 0.36)) and minimal change (35.2%; -0.20 (-0.21, -0.19)). Results were similar when stratified by primary diagnosis of upper extremity, lower extremity or spine conditions, with small differences in the relative proportion of trajectory class membership by body region. Predictive factors for less favourable disability trajectories included older age, lower physical and mental health scores, body region, higher social deprivation index, insurance type and certain comorbidities.
Conclusions: Most patients showed improvement in disability after exposure to treatment by a physical therapist, but a notable proportion experienced minimal change or worsening. Multiple demographic, physical, mental and social health factors differentiated trajectory class membership, highlighting opportunities to improve how and to whom this type of guideline-supported non-pharmacological care is delivered.
Keywords: Clinical Reasoning; Health Services; Musculoskeletal disorders; PAIN MANAGEMENT; Patient Reported Outcome Measures; REHABILITATION MEDICINE.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: CT and AL are employees of ATI Physical Therapy. TL is an unpaid Advisory Board member for the Institute of Musculoskeletal Advancement (iMSKA). SZG receives honorarium from the American Physical Therapy Association for his Editor role with the Physical Therapy & Rehabilitation journal. All other authors have no competing interest to declare.
Figures
Similar articles
-
How lived experiences of illness trajectories, burdens of treatment, and social inequalities shape service user and caregiver participation in health and social care: a theory-informed qualitative evidence synthesis.Health Soc Care Deliv Res. 2025 Jun;13(24):1-120. doi: 10.3310/HGTQ8159. Health Soc Care Deliv Res. 2025. PMID: 40548558
-
Exercise for intermittent claudication.Cochrane Database Syst Rev. 2017 Dec 26;12(12):CD000990. doi: 10.1002/14651858.CD000990.pub4. Cochrane Database Syst Rev. 2017. PMID: 29278423 Free PMC article.
-
Quality improvement strategies for diabetes care: Effects on outcomes for adults living with diabetes.Cochrane Database Syst Rev. 2023 May 31;5(5):CD014513. doi: 10.1002/14651858.CD014513. Cochrane Database Syst Rev. 2023. PMID: 37254718 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Exercise for hand osteoarthritis.Cochrane Database Syst Rev. 2017 Jan 31;1(1):CD010388. doi: 10.1002/14651858.CD010388.pub2. Cochrane Database Syst Rev. 2017. PMID: 28141914 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources