

Economic evaluation of inpatient medication reconciliation with a subtraction strategy
- PMID: 40542934
- PMCID: PMC12181825
- DOI: 10.1186/s13561-025-00649-0
Economic evaluation of inpatient medication reconciliation with a subtraction strategy
Abstract
Background: University-based hospitals in Thailand face increasing financial strain due to insufficient reimbursement for inpatient care. The public health financing system comprises three major schemes: the Universal Coverage Scheme (UCS), Social Security Scheme (SSS), and Civil Servant Medical Benefit Scheme (CSMBS), which differ in funding mechanisms and reimbursement rates. Although all schemes apply the Diagnosis-Related Groups (DRG) system for inpatient payment, variations in base rates and case-mix complexity often leave tertiary hospitals underfunded. Medication reconciliation (MR) with a subtraction strategy-deducting patients' home medications from discharge prescriptions-has been implemented to optimize hospital resources. This study aimed to evaluate cost savings and identify key determinants influencing the economic outcomes of MR across public insurance schemes.
Methods: We conducted a retrospective cohort study of 563 hospitalized internal medicine patients at a university-based hospital. Of these, 324 underwent MR with subtraction. Cost savings and reimbursement margins were calculated from the provider's perspective. Patients were stratified by healthcare scheme (CSMBS, UCS, SSS) and length of stay (LOS). Generalized Linear Mixed Models were used to identify factors associated with cost savings.
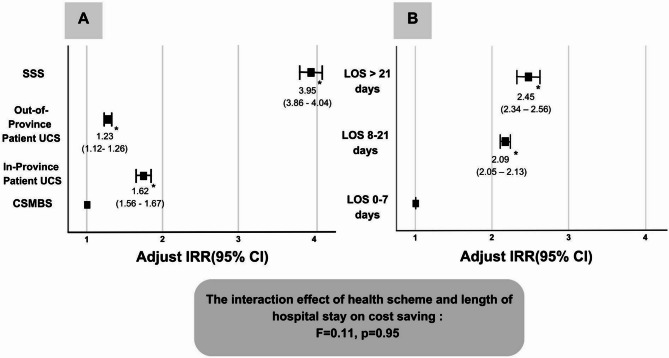
Results: The highest mean cost savings per patient were observed in the SSS group (508.5 ± 56.1 THB [~ 14.1 USD]), and the lowest in CSMBS (133.5 ± 23.6 THB [~ 3.7 USD]). Prolonged LOS was associated with significantly greater savings (LOS > 21 days: IRR = 2.45, p < 0.001). SSS patients achieved the greatest overall savings (IRR = 3.95, p < 0.001). Nonetheless, negative reimbursement margins persisted across all schemes.
Conclusions: Although MR with subtraction achieved measurable cost savings, it failed to offset reimbursement deficits. Broader financial reforms are needed to ensure sustainability, with MR positioned as a potentially scalable strategy within value-based care frameworks.
Keywords: Cost minimization; Economic efficiency; Hospital policy; Medication reconciliation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Approved by the Human Research Ethics Committee (EC-67-140) and conducted per the Declaration of Helsinki. Disclaimer: The views expressed are those of the authors, not necessarily of the funding agency. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.Health Technol Assess. 2006 Aug;10(28):iii-iv, xi-xiv, 1-183. doi: 10.3310/hta10280. Health Technol Assess. 2006. PMID: 16904047
References
-
- Chang A, Schyve PM, Croteau RJ, O’Leary DS, Loeb JM. The JCAHO patient safety event taxonomy: a standardized terminology and classification schema for near misses and adverse events. Int J Qual Health Care. 2005;17(2):95–105. - PubMed
-
- Bruning K, Selder F. From hospital to home healthcare: the need for medication reconciliation. Home Healthc now. 2011;29(2):81–90. - PubMed
-
- World Health Organization. The Kingdom of Thailand health system review. Health Syst Transition. 2015;5(5).
-
- Kohler JC, Ovtcharenko N. Good governance for medicines initiatives: exploring lessons learned. U4 Issue. 2013.
Grants and funding
LinkOut - more resources
Full Text Sources
