

Modeling gonorrhea vaccination to find optimal targeting strategies that balance impact with cost-effectiveness
- PMID: 40544168
- PMCID: PMC12182581
- DOI: 10.1038/s41541-025-01159-0
Modeling gonorrhea vaccination to find optimal targeting strategies that balance impact with cost-effectiveness
Abstract
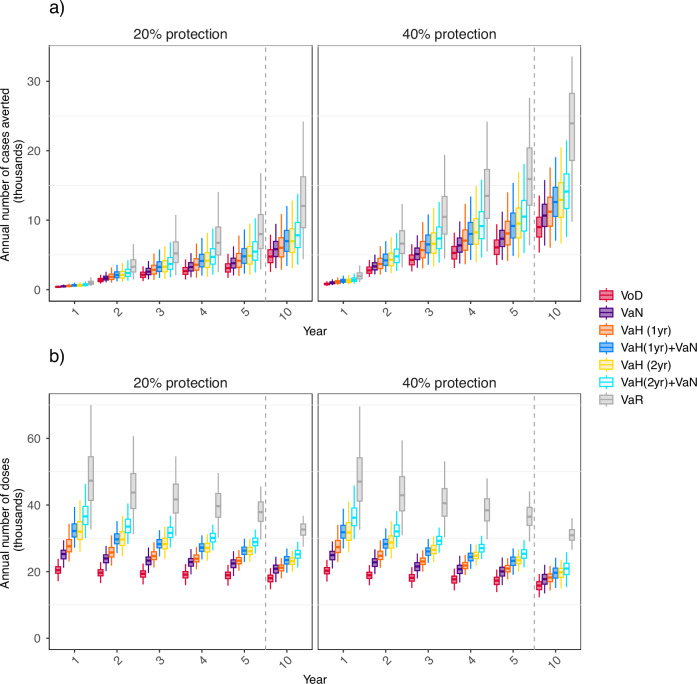
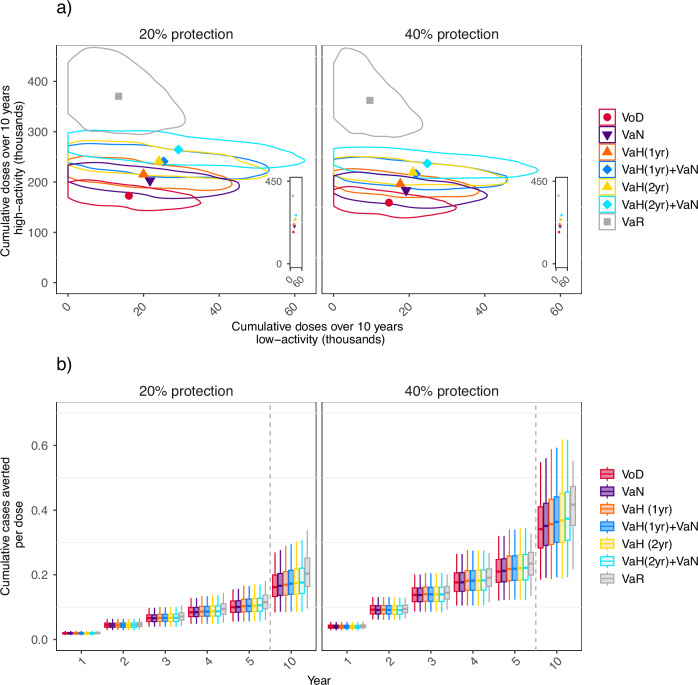
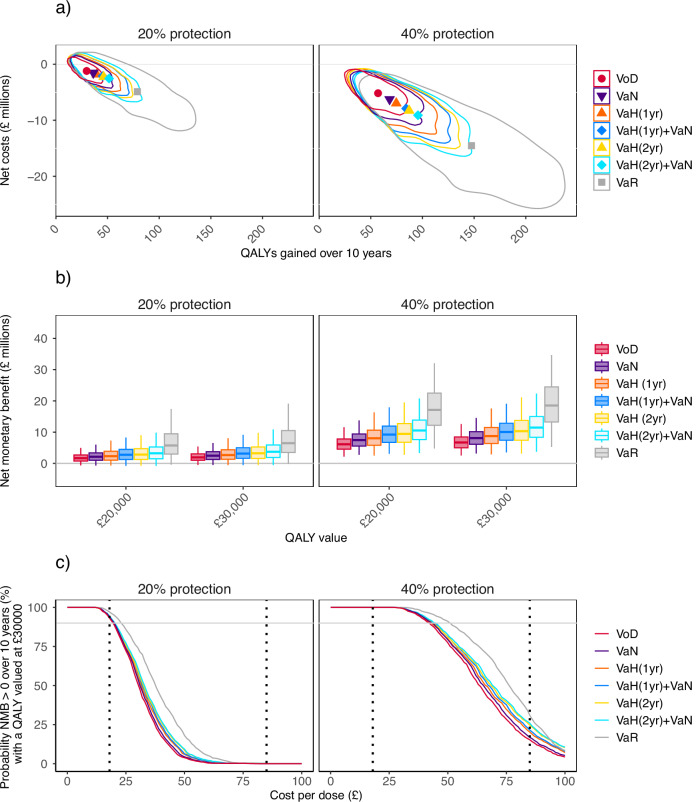
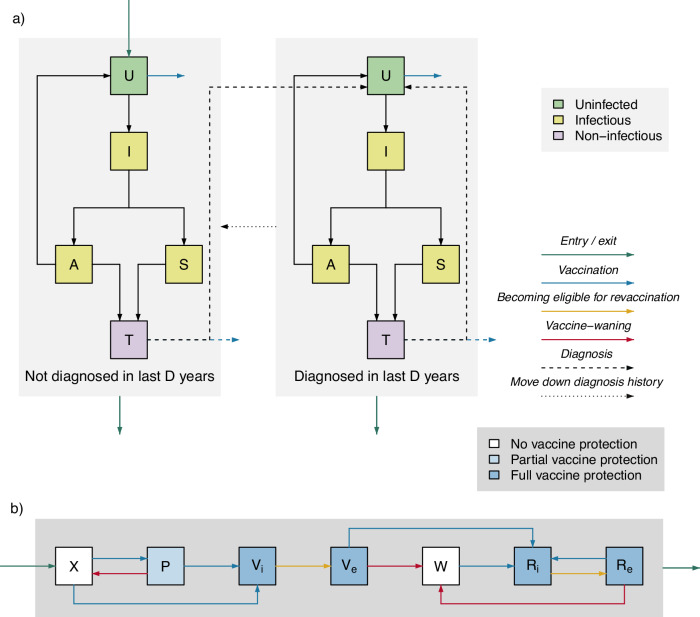
Vaccination for UK men who have sex with men (MSM) at increased gonorrhea risk has been advised, but not yet implemented. Effective targeting is essential for cost-effectiveness, but previously-examined approaches have disadvantages: Vaccination-on-Diagnosis has low coverage (limiting impact), and Vaccination-according-to-Risk requires asking about sexual behavior to identify at-risk individuals, which is not always feasible. We developed a transmission-dynamic model to evaluate novel strategies offering vaccination based on information readily available to clinicians (diagnostic/vaccination history, if the patient is seeking care due to partner notification). Offering vaccination to MSM who are notified partners of gonorrhea cases or were diagnosed themselves in the past 2 years averts 1.6x more cases and is more cost-effective than Vaccination-on-Diagnosis. If vaccination provides 20% protection for 1.5 years after primary vaccination and 3 years after revaccination then at £18/dose administered, all considered strategies have ≥50 and ≥90% probabilities of positive net monetary benefit compared with no vaccination with a quality-adjusted life year valued at £20,000 and £30,000 respectively, thus meeting the UK criteria for cost-effectiveness. All novel strategies considered achieve greater impact than Vaccination-on-Diagnosis without the feasibility issues of Vaccination-according-to-Risk.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: L.K.W. has consulted for the Wellcome Trust. P.J.W. has received payment from Pfizer for teaching of mathematical modeling of infectious disease transmission and vaccination, and from the Dutch National Institute for Public Health and the Environment (RIVM) for participation in an audit committee on COVID-19 data analytics and modeling. T.L. and D.N. report no potential conflicts.
Figures
Similar articles
-
Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men.Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001230. doi: 10.1002/14651858.CD001230.pub2. Cochrane Database Syst Rev. 2008. PMID: 18646068
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
Surveillance of Barrett's oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.Health Technol Assess. 2006 Mar;10(8):1-142, iii-iv. doi: 10.3310/hta10080. Health Technol Assess. 2006. PMID: 16545207
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
Cited by
-
Comparing Strategies to Introduce Two New Antibiotics for Gonorrhea: A Modeling Study.medRxiv [Preprint]. 2025 Jul 3:2025.07.01.25330638. doi: 10.1101/2025.07.01.25330638. medRxiv. 2025. PMID: 40630587 Free PMC article. Preprint.
References
-
- World Health Organization. Multi-drug resistant gonorrhoea. https://www.who.int/news-room/fact-sheets/detail/multi-drug-resistant-go... (2024).
-
- Tacconelli, E. et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis.18, 318–327 (2018). - PubMed
-
- Unemo, M. et al. Sexually transmitted infections: challenges ahead. Lancet Infect. Dis.17, e235–e279 (2017). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
