

Prediction of risk factors of plastic bronchitis in children with severe Mycoplasma pneumoniae pneumonia
- PMID: 40544237
- PMCID: PMC12181858
- DOI: 10.1186/s12938-025-01410-8
Prediction of risk factors of plastic bronchitis in children with severe Mycoplasma pneumoniae pneumonia
Abstract
Background: Plastic bronchitis (PB) is a rare but potentially life-threatening condition that requires particular attention in pediatric patients, specifically those presenting with severe Mycoplasma pneumoniae pneumonia (SMPP). This study aimed to identify risk factors associated with PB in children with SMPP and develop a comprehensive risk factor scoring system.
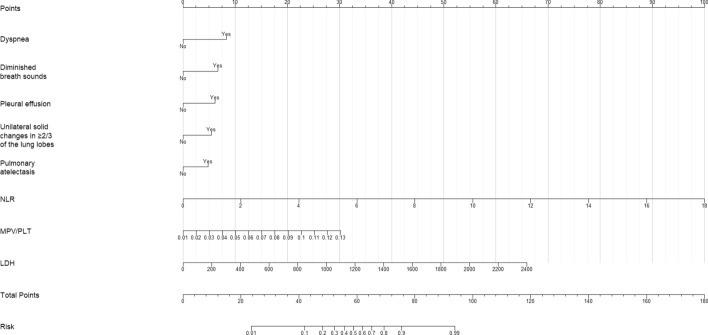
Methods: A retrospective analysis was conducted on SMPP patients who underwent bronchoscopy between January 2018 and October 2023. Based on bronchoscopic and pathological examination results, patients were categorized into PB (n = 142) and non-PB (n = 274) groups. Clinical manifestations, laboratory data, and imaging findings were analyzed. Risk factors for PB in SMPP children were identified through univariate and multivariate logistic regression analyses. A nomogram model incorporating independent risk factors was developed, and a PB risk factor scoring system was established. Model validation was performed through a prospective validation study.
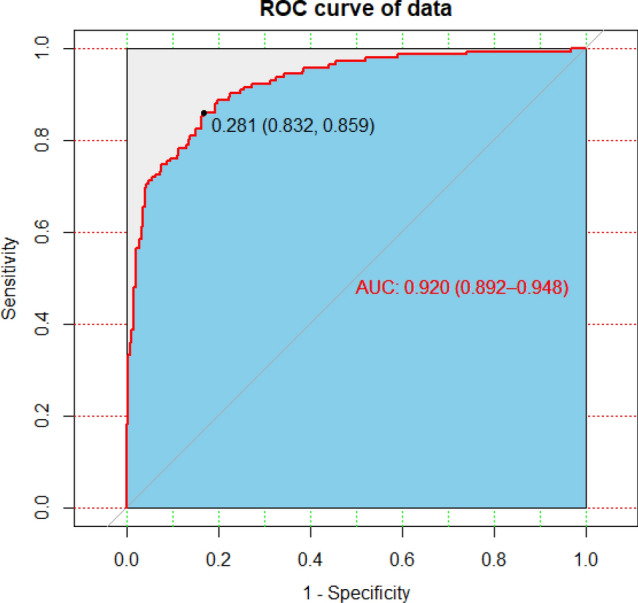
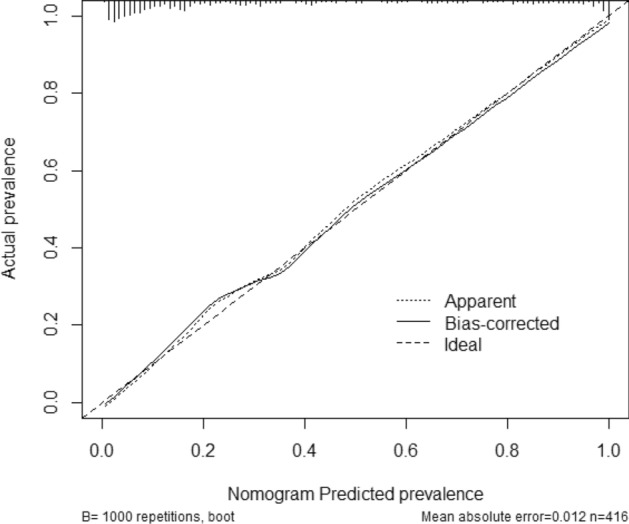
Results: Among 416 SMPP children (197 males, 219 females), mean age at disease onset was 6.9 ± 2.9 years and 6.6 ± 2.8 years in the PB and Non-PB groups, respectively. Multivariate logistic regression analysis identified eight independent predictors of PB in SMPP children: dyspnea, decreased breath sounds, neutrophil-to-lymphocyte ratio (NLR), lactate dehydrogenase (LDH), mean platelet volume to platelet ratio (MPV/PLT), pleural effusion, ≥ 2/3 lobe consolidation, and atelectasis. The nomogram prediction model demonstrated excellent discriminative ability (AUC = 0.92, 95% CI 0.892-0.948, P < 0.005) and strong calibration between predicted and observed outcomes. In the prospective validation cohort (n = 565), the scoring system effectively stratified patients into risk categories: high-risk (71.62% PB incidence), intermediate-risk (59.79%), and low-risk (5.33%), with statistically significant inter-group differences (P < 0.001). The PB group exhibited significantly longer hospitalization durations, extended glucocorticoid treatment periods, higher proportions of glucocorticoid therapy utilization, and a greater frequency of bronchoscopy interventions (≥ 2 sessions) compared to the Non-PB group (all P < 0.05).
Conclusions: In this study, we developed and validated a nomogram to PB in children with SMPP. This model serves as a clinically practical tool for early PB identification, enabling physicians to initiate timely interventions and optimize disease management strategies.
Keywords: Children; Nomogram; Plastic bronchitis; Prediction model; Risk factors; Severe Mycoplasma pneumoniae pneumonia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics statement and consent to participate: This investigation was conducted in accordance with the Declaration of Helsinki (2013 revision) and received approval from the Institutional Ethics Committee of Tianjin Children's Hospital (Approval number:2022-LXKY-008). The requirement for written informed consent was waived due to the retrospective nature of the initial analysis, with all patient data anonymized prior to evaluation. Consent for publication: Not applicable. Competing interests: The authors declare no actual or potential competing financial interests.
Figures
References
-
- Cai X, Sun J, Li W, Cheng H. Clinical analysis of severe plastic bronchitis in 8 children. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28(1):73–5. - PubMed
-
- Su M, Wang Q, Li D, Wang LL, Wang CY, Wang JL, et al. Prevalence and clinical characteristics of hospitalized children with community-acquired Mycoplasma pneumoniae pneumonia during 2017/2018, Chengde, China. Medicine. 2021;100(5): e23786. 10.1097/MD.0000000000023786.PMID:33592835;PMCID:PMC7870167. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
