

The nexus between healthcare provider distribution and neonatal mortality based on the context of maternal and child healthcare services in Pakistan
- PMID: 40544296
- PMCID: PMC12181886
- DOI: 10.1186/s41043-025-00971-7
The nexus between healthcare provider distribution and neonatal mortality based on the context of maternal and child healthcare services in Pakistan
Abstract
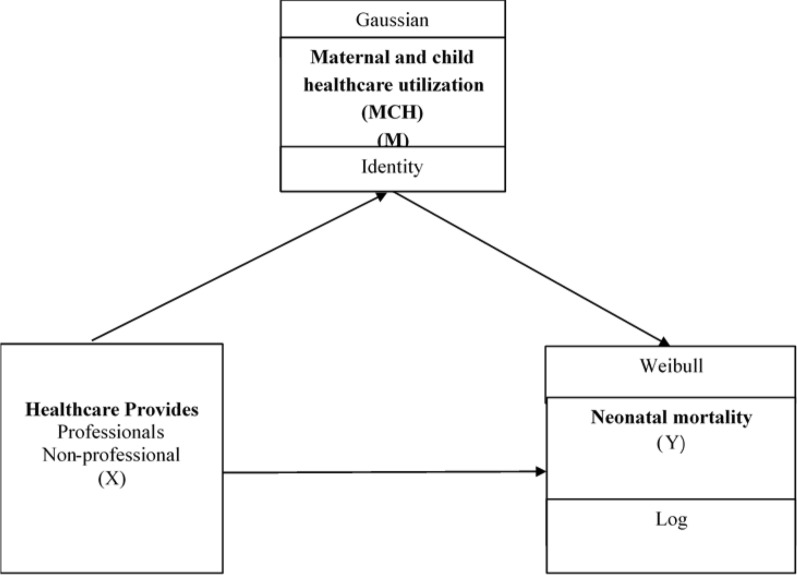
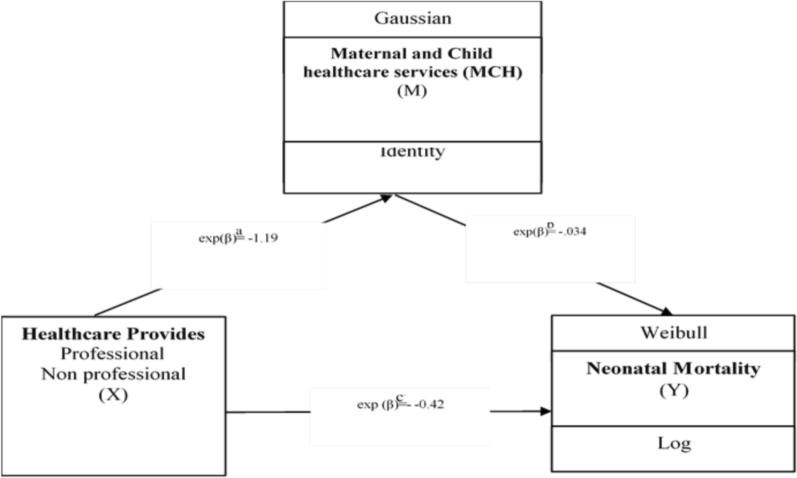
Background: Healthcare provider dearth, particularly in Low and Middle-income countries (LMICs), reduces the development towards improved healthcare outcomes and accomplish the Sustainable Development Goals (SDGs-3). This study aims to investigate the association between Professional and Non-professional healthcare provider distribution and neonatal mortality through the mediating role of maternal and child healthcare (MCH) services in Pakistan.
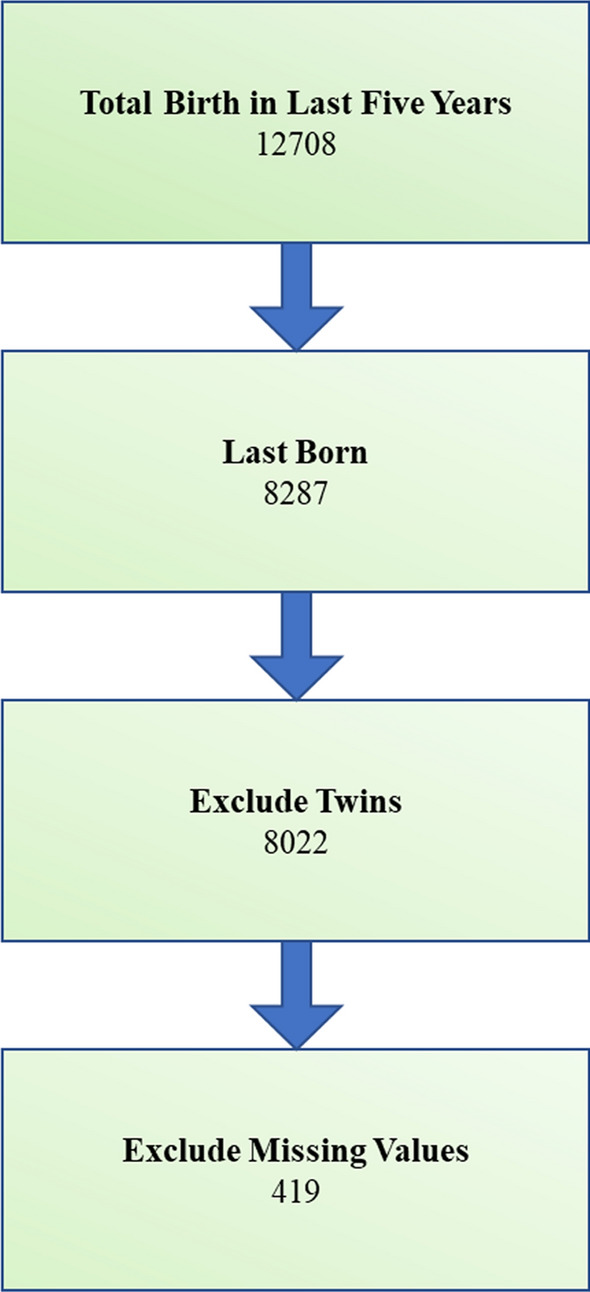
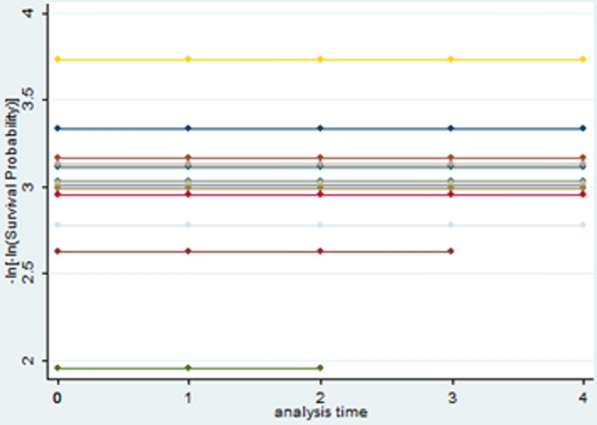
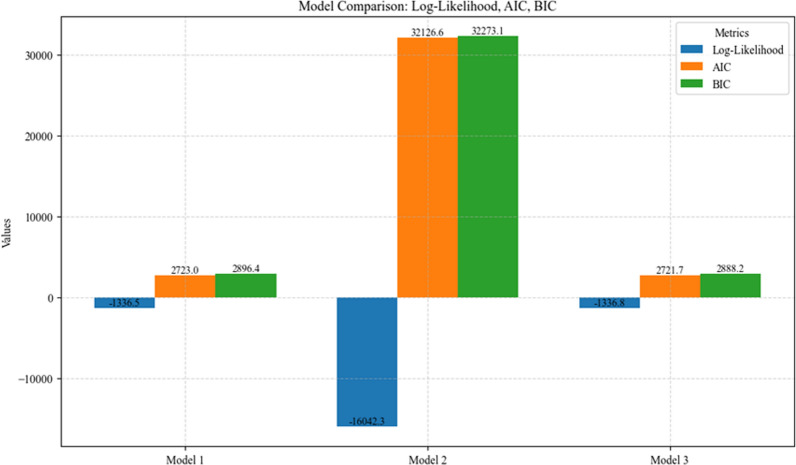
Methods: The present research used data from the 2018 Pakistan Demographic and Health Survey (PDHS) total sample that comprises (N = 8022). The dependent variable includes the risk of neonatal mortality 0-30 days. Bivariate and Multivariate analyses were conducted by utilizing the Cox proportional hazards and regression models. The estimation of mortality rates was achieved through generalized structural equation modelling (GSEM) and the 5000 bootstrap technique. All the investigations were carried out in STATA v. 16.1.
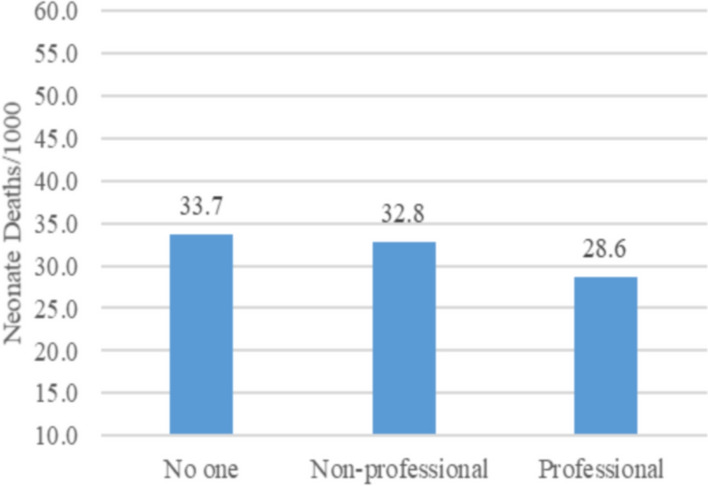
Results: Our results revealed that around 2.46% of neonatal deaths occur. The average healthcare provider distribution type was professional, 83.45%, non-professional, 1.45%, and no care, 15.11%. 0.88% of females are less likely to die within the first thirty days of their birth compared to males. The regression outcomes demonstrate that the healthcare providers were positive and significantly linked to neonatal mortality. Additionally, a unit increase in healthcare providers has a 1.20% Higher likelihood of increasing the MCH and overall reducing neonatal mortality (HR = 0.60).
Conclusion: The outcomes illustrate that healthcare provider distribution and MCH play a vital role in minimizing neonatal mortality. To ensure well-distributed healthcare provider distribution, promoting maternal education, empowering women's decision-making in acquiring MCH services utilization, and expanding access to free MCH services are the essentials for better maternal and healthcare outcomes.
Keywords: Child health services; Developing countries; Generalized structural equation modelling; Healthcare workforce; Maternal health services; Mortality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study involves human participants and procedures, and questionnaires for standard DHS surveys have been reviewed and approved by the ICF Institutional Review Board (IRB). Additionally, country-specific DHS survey protocols are reviewed by the ICF IRB and typically by an IRB in the host country. ICF IRB ensures that the survey complies with the US Department of Health and Human Services regulations for protecting human subjects (45 CFR 46), while the host country IRB ensures that the survey complies with the laws and norms of the nation. Participants gave informed consent to participate in the study before taking part. Consent for publication: Not applicable. Patient and public involvement: Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Effects of consumers and health providers working in partnership on health services planning, delivery and evaluation.Cochrane Database Syst Rev. 2021 Sep 15;9(9):CD013373. doi: 10.1002/14651858.CD013373.pub2. Cochrane Database Syst Rev. 2021. PMID: 34523117 Free PMC article.
-
Family-centred interventions for Indigenous early childhood well-being by primary healthcare services.Cochrane Database Syst Rev. 2022 Dec 13;12(12):CD012463. doi: 10.1002/14651858.CD012463.pub2. Cochrane Database Syst Rev. 2022. PMID: 36511823 Free PMC article.
-
Non-clinical interventions for reducing unnecessary caesarean section.Cochrane Database Syst Rev. 2018 Sep 28;9(9):CD005528. doi: 10.1002/14651858.CD005528.pub3. Cochrane Database Syst Rev. 2018. PMID: 30264405 Free PMC article.
-
Shared decision-making interventions for people with mental health conditions.Cochrane Database Syst Rev. 2022 Nov 11;11(11):CD007297. doi: 10.1002/14651858.CD007297.pub3. Cochrane Database Syst Rev. 2022. PMID: 36367232 Free PMC article.
-
Multiple-micronutrient supplementation for women during pregnancy.Cochrane Database Syst Rev. 2017 Apr 13;4(4):CD004905. doi: 10.1002/14651858.CD004905.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2019 Mar 14;3:CD004905. doi: 10.1002/14651858.CD004905.pub6. PMID: 28407219 Free PMC article. Updated.
References
-
- Bhowmik J, Apputhurai P, Williams J, Biswas RK. Investigating the role of women’s education status and empowerment on accessing skilled birth attendance in Bangladesh: a structural equation modelling approach. Midwifery. 2024;1(138):104140. - PubMed
-
- Altuhaifa F, Al TM. Machine learning models for predicting missing gender in cancer data. Int J Data Sci Anal. 2025;28:1–5.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
